

Radiologic Findings and Patient Factors Associated with 30-Day Mortality after Surgical Evacuation of Subdural Hematoma in Patients Less Than 65 Years Old
- PMID: 28264246
- PMCID: PMC5365301
- DOI: 10.3340/jkns.2016.0404.009
Radiologic Findings and Patient Factors Associated with 30-Day Mortality after Surgical Evacuation of Subdural Hematoma in Patients Less Than 65 Years Old
Abstract
Objective: The purpose of this study is to evaluate the associations between 30-day mortality and various radiological and clinical factors in patients with traumatic acute subdural hematoma (SDH). During the 11-year study period, young patients who underwent surgery for SDH were followed for 30 days. Patients who died due to other medical comorbidities or other organ problems were not included in the study population.
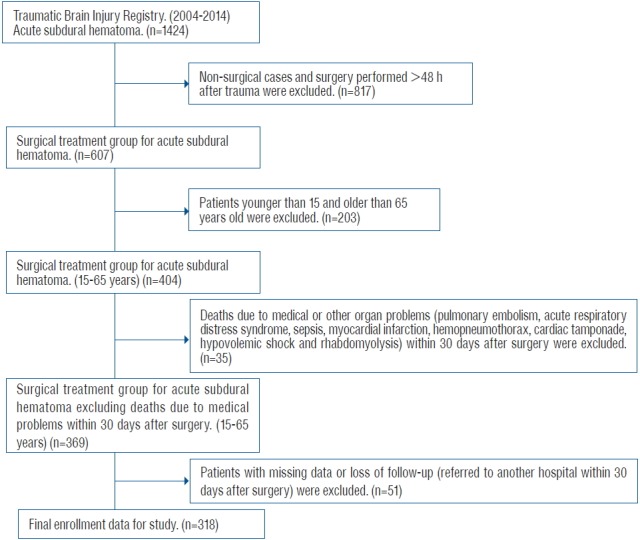
Methods: From January 1, 2004 to December 31, 2014, 318 consecutive surgically-treated traumatic acute SDH patients were registered for the study. The Kaplan-Meier method was used to analyze 30-day survival rates. We also estimated the hazard ratios of various variables in order to identify the independent predictors of 30-day mortality.
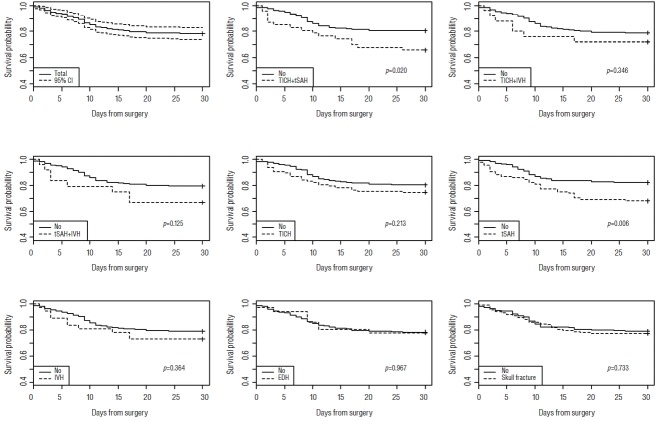
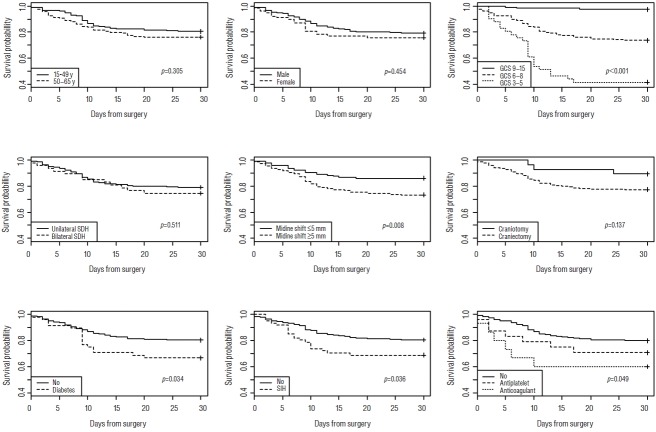
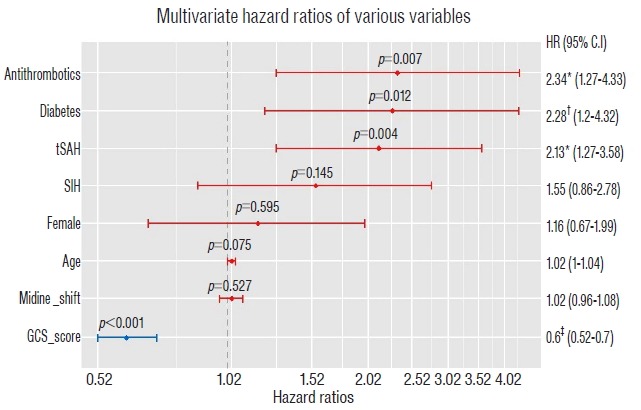
Results: We observed a negative correlation between 30-day mortality and Glasgow coma scale score (per 1-point score increase) (hazard ratio [HR], 0.60; 95% confidence interval [CI], 0.52-0.70; p<0.001). In addition, use of antithrombotics (HR, 2.34; 95% CI, 1.27-4.33; p=0.008), history of diabetes mellitus (HR, 2.28; 95% CI, 1.20-4.32; p=0.015), and accompanying traumatic subarachnoid hemorrhage (hazard ratio, 2.13; 95% CI, 1.27-3.58; p=0.005) were positively associated with 30-day mortality.
Conclusion: We found significant associations between short-term mortality after surgery for traumatic acute SDH and lower Glasgow Coma Scale scores, use of antithrombotics, history of diabetes mellitus, and accompanying traumatic subarachnoid hemorrhage at admission. We expect these findings to be helpful for selecting patients for surgical treatment of traumatic acute SDH, and for making accurate prognoses.
Keywords: Mortality; Subdural hematoma; Traumatic brain injury; Traumatic subarachnoid hemorrhage.
Figures
Similar articles
-
Nonsurgical acute traumatic subdural hematoma: what is the risk?J Neurosurg. 2015 Nov;123(5):1176-83. doi: 10.3171/2014.10.JNS141728. Epub 2015 May 8. J Neurosurg. 2015. PMID: 25955872
-
Subdural hematoma as a major determinant of short-term outcomes in traumatic brain injury.J Neurosurg. 2018 Jan;128(1):236-249. doi: 10.3171/2016.5.JNS16255. Epub 2017 Feb 10. J Neurosurg. 2018. PMID: 28186445
-
Adverse Outcomes After Initial Non-surgical Management of Subdural Hematoma: A Population-Based Study.Neurocrit Care. 2016 Apr;24(2):226-32. doi: 10.1007/s12028-015-0178-x. Neurocrit Care. 2016. PMID: 26160466
-
The Outcomes of Traumatic Acute Subdural Hematoma in a Tertiary Center in Abuja, Nigeria.Cureus. 2021 Nov 29;13(11):e20016. doi: 10.7759/cureus.20016. eCollection 2021 Nov. Cureus. 2021. PMID: 34987904 Free PMC article.
-
Surgical management of acute subdural hematomas.Neurosurgery. 2006 Mar;58(3 Suppl):S16-24; discussion Si-iv. Neurosurgery. 2006. PMID: 16710968 Review.
Cited by
-
Traumatic brain injury: Association between the Glasgow Coma Scale score and intensive care unit mortality.South Afr J Crit Care. 2022 Aug 5;38(2):10.7196/SAJCC.2022.v38i2.525. doi: 10.7196/SAJCC.2022.v38i2.525. eCollection 2022. South Afr J Crit Care. 2022. PMID: 36101711 Free PMC article.
-
Comorbidity in adults with traumatic brain injury and all-cause mortality: a systematic review.BMJ Open. 2019 Nov 7;9(11):e029072. doi: 10.1136/bmjopen-2019-029072. BMJ Open. 2019. PMID: 31699721 Free PMC article.
References
-
- Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg. 2006;104:469–479. - PubMed
-
- Beynon C, Potzy A, Sakowitz OW, Unterberg AW. Rivaroxaban and intracranial haemorrhage after mild traumatic brain injury: A dangerous combination? Clin Neurol Neurosurg. 2015;136:73–78. - PubMed
-
- Bosarge PL, Shoultz TH, Griffin RL, Kerby JD. Stress-induced hyperglycemia is associated with higher mortality in severe traumatic brain injury. J Trauma Acute Care Surg. 2015;79:289–294. - PubMed
-
- Cepeda S, Gómez PA, Castaño-Leon AM, Martínez-Pérez R, Munarriz PM, Lagares A. Traumatic intracerebral hemorrhage: risk factors associated with progression. J Neurotrauma. 2015;32:1246–1253. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
