

Duration of veno-arterial extracorporeal life support (VA ECMO) and outcome: an analysis of the Extracorporeal Life Support Organization (ELSO) registry
- PMID: 28264702
- PMCID: PMC5339999
- DOI: 10.1186/s13054-017-1633-1
Duration of veno-arterial extracorporeal life support (VA ECMO) and outcome: an analysis of the Extracorporeal Life Support Organization (ELSO) registry
Abstract
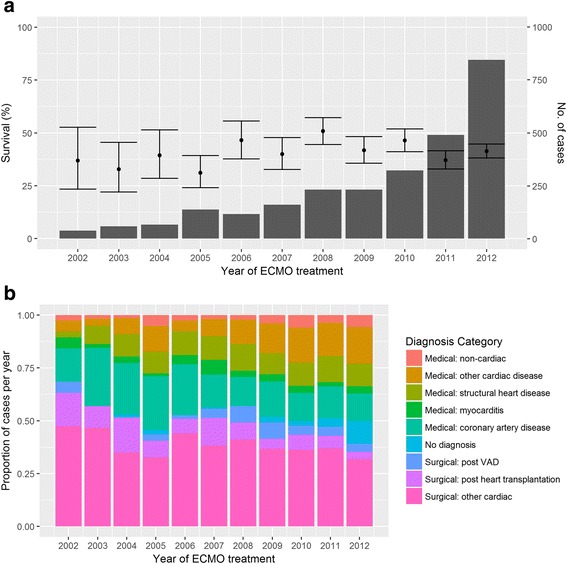
Background: Veno-arterial extracorporeal membrane oxygenation (VA ECMO) is an effective rescue therapy for severe cardiorespiratory failure, but morbidity and mortality are high. We hypothesised that survival decreases with longer VA ECMO treatment. We examined the Extracorporeal Life Support Organization (ELSO) registry for a relationship between VA ECMO duration and in-hospital mortality, and covariates including indication for support.
Methods: All VA runs from the ELSO database from 2002 to 2012 were extracted. Multiple runs and non-VA runs were excluded. Runs were categorized into diagnostic groups. Logistic regression for analysis of the effect of duration on outcome, and multivariate regression for diagnosis and other baseline factors were performed. Non-linear models including piecewise logistic models were fitted.
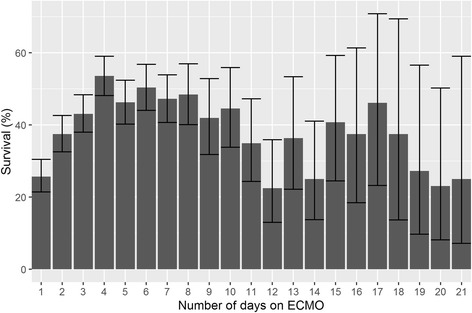
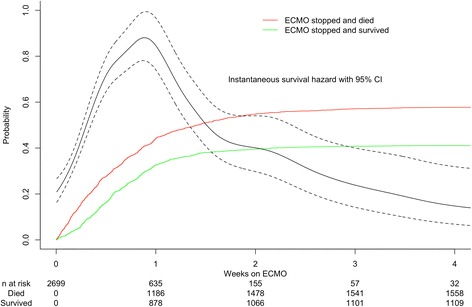
Results: There were 2699 runs analysed over 14,747 days. Logistic regression analysis of the effect of duration on outcome, and multivariate regression analysis of diagnosis and other baseline factors were performed. In-hospital survival was 41.4% (95% CI 39.6-43.3). 75% of patients were supported for less than 1 week and 96% for less than 3 weeks. Median duration (4 days IQR 2.0-6.8) was greater in survivors (4.1 (IQR 2.5-6.7) vs 3.8 (IQR 1.7-7.0) p = 0.002). The final multivariate model demonstrated increasing survival to day 4 (OR 1.53 (95% CI 1.37-1.71) p < 0.001), decreasing from day 4 to 12 (OR 0.86 (95% CI 0.81-0.91), p < 0.001) with no significant change thereafter (OR 0.98 (95% CI 0.94-1.02), p = 0.400).
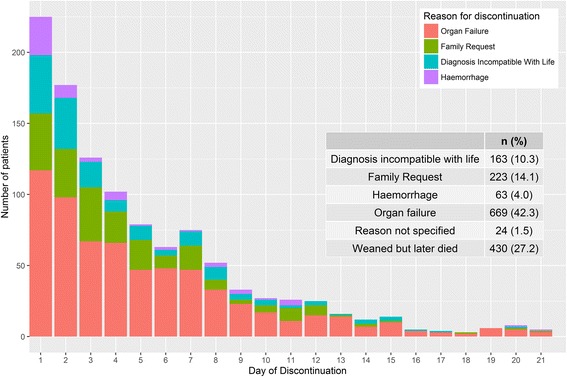
Conclusions: ECMO for 4 days or less is associated with higher mortality, likely reflecting early treatment failure. Survival is highest when patients are weaned on the fourth day of ECMO but likely decreases into the second week. While this does not suggest weaning at this point will produce better outcomes, it does reflect the likely time course of ECMO as a bridge in severe shock. Patients with some underlying conditions (like myocarditis and heart transplantation) achieve better outcomes despite longer support duration. These findings merit prospective study for the development of prognostic models and weaning strategies.
Keywords: Extracorporeal Life Support Organization; Extracorporeal membrane oxygenation; Outcomes; Refractory shock; Survival; Treatment duration.
Figures
Comment in
-
Confounding variables impacting the association between duration of veno-arterial extracorporeal life support and mortality.Crit Care. 2017 Aug 1;21(1):203. doi: 10.1186/s13054-017-1773-3. Crit Care. 2017. PMID: 28764805 Free PMC article. No abstract available.
References
-
- Extracorporeal Life Support Organization - ECMO and ECLS > Registry > Statistics > International Summary. 2016. https://www.elso.org/Registry/Statistics/InternationalSummary.aspx. Accessed 6 May 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
