

Retrospective review of Surgical Availability and Readiness in 8 African countries
- PMID: 28264832
- PMCID: PMC5353330
- DOI: 10.1136/bmjopen-2016-014496
Retrospective review of Surgical Availability and Readiness in 8 African countries
Abstract
Objectives: The purpose of this study was to assess surgical availability and readiness in 8 African countries using the WHO's Service Availability and Readiness Assessment (SARA) tool.
Setting: We analysed data for surgical services, including basic and comprehensive surgery, comprehensive obstetric care, blood transfusion, and infection prevention, obtained from the WHO's SARA surveys in Sierra Leone, Uganda, Mauritania, Benin, Zambia, Burkina Faso, Democratic Republic of Congo and Togo.
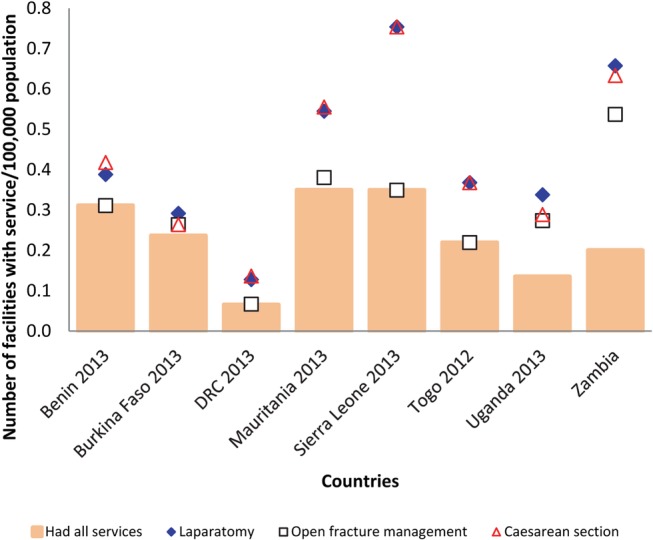
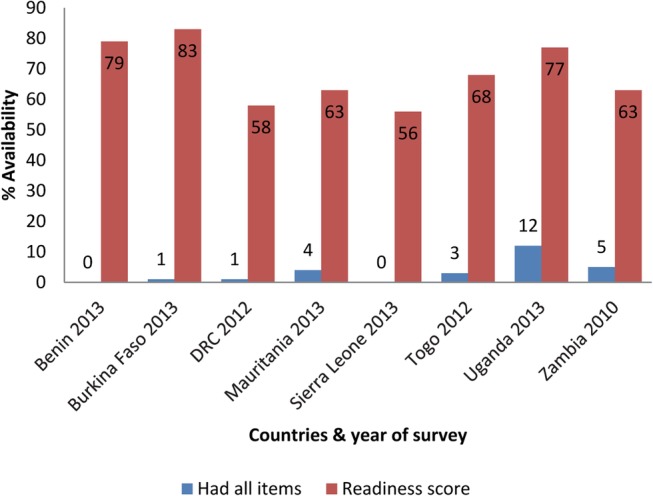
Primary and secondary outcome measures: Among the facilities that were expected to offer surgical services (N=3492), there were wide disparities between the countries in the number of facilities per 100 000 population that reported offering basic surgery (1.0-12.1), comprehensive surgery (0.1-0.8), comprehensive obstetric care (0.1-0.8) and blood transfusion (0.1-0.8). Only 0.1-0.3 facilities per 100 000 population had all three bellwether procedures available, namely laparotomy, open fracture management and caesarean section. In all the countries, the facilities that reported offering surgical services generally had a shortage of the necessary items for offering the services and this varied greatly between the countries, with the facilities having on average 27-53% of the items necessary for offering basic surgery, 56-83% for comprehensive surgery, 49-72% for comprehensive obstetric care and 54-80% for blood transfusion. Furthermore, few facilities had all the necessary items present. However, facilities that reported offering surgical services had on average most of the necessary items for the prevention of infection.
Conclusions: There are important gaps in the surgical services in the 8 African countries surveyed. Efforts are therefore urgently needed to address deficiencies in the availability and readiness to deliver surgical services in these nations, and this will require commitment from multiple stakeholders. SARA may be used to monitor availability and readiness at regular intervals, which will enable stakeholders to evaluate progress and identify gaps and areas for improvement.
Keywords: Africa; Deficiencies; SARA; Surgical services.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Figures






Similar articles
-
Assessment of Family Planning Service Availability and Readiness in 10 African Countries.Glob Health Sci Pract. 2018 Oct 4;6(3):473-483. doi: 10.9745/GHSP-D-18-00041. Print 2018 Oct 3. Glob Health Sci Pract. 2018. PMID: 30213877 Free PMC article.
-
Linking household and health facility surveys to assess obstetric service availability, readiness and coverage: evidence from 17 low- and middle-income countries.J Glob Health. 2018 Jun;8(1):010603. doi: 10.7189/jogh.08.010603. J Glob Health. 2018. PMID: 29862026 Free PMC article.
-
Summary of country-level activities in population education in the African region: Unesco experience.Educafrica. 1985 Jun;(12):199-207. Educafrica. 1985. PMID: 12268119
-
Optimizing the management of acute coronary syndromes in sub-Saharan Africa: A statement from the AFRICARDIO 2015 Consensus Team.Arch Cardiovasc Dis. 2016 Jun-Jul;109(6-7):376-83. doi: 10.1016/j.acvd.2015.12.005. Epub 2016 Mar 25. Arch Cardiovasc Dis. 2016. PMID: 27020513
-
Revisiting sub-Saharan African countries' drug problems: health, social, economic costs, and drug control policy.Subst Use Misuse. 2002 Feb;37(3):265-90. doi: 10.1081/ja-120002479. Subst Use Misuse. 2002. PMID: 11913904 Review.
Cited by
-
Access to Orthopaedic Surgical Care in Northern Tanzania: A Modelling Study.World J Surg. 2018 Oct;42(10):3081-3088. doi: 10.1007/s00268-018-4630-x. World J Surg. 2018. PMID: 29696326
-
Assessing service availability and readiness to manage Chronic Respiratory Diseases (CRDs) in Bangladesh.PLoS One. 2021 Mar 4;16(3):e0247700. doi: 10.1371/journal.pone.0247700. eCollection 2021. PLoS One. 2021. PMID: 33661982 Free PMC article.
-
Challenges and solutions to providing surgery in Sierra Leone hospitals: a qualitative analysis of surgical provider perspectives.BMJ Open. 2022 Feb 1;12(2):e052972. doi: 10.1136/bmjopen-2021-052972. BMJ Open. 2022. PMID: 35105579 Free PMC article.
-
Health facilities' readiness for safe surgical care provision in Uganda and the Eastern Democratic Republic of Congo during Ebola and COVID-19 era.BMC Health Serv Res. 2021 Aug 18;21(1):831. doi: 10.1186/s12913-021-06870-x. BMC Health Serv Res. 2021. PMID: 34404419 Free PMC article.
-
Blood transfusion service readiness and its associated factors in health facilities providing blood transfusion services across Ethiopia: A secondary analysis of the 2018 Service Availability and Readiness Assessment (SARA) survey.PLoS One. 2024 Dec 12;19(12):e0315665. doi: 10.1371/journal.pone.0315665. eCollection 2024. PLoS One. 2024. PMID: 39666720 Free PMC article.
References
-
- Debas HT, Donkor P, Gawande A et al. In: Jamison DT, Kruk ME, Mock CN, eds. Essential surgery: disease control priorities. 3rd edn (Vol 1). Washington DC: The International Bank for Reconstruction and Development / The World Bank, 2015:19–40. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources