

Incident Coronary Heart Disease After Preeclampsia: Role of Reduced Fetal Growth, Preterm Delivery, and Parity
- PMID: 28264858
- PMCID: PMC5523993
- DOI: 10.1161/JAHA.116.004158
Incident Coronary Heart Disease After Preeclampsia: Role of Reduced Fetal Growth, Preterm Delivery, and Parity
Abstract
Background: Preeclampsia is a severe pregnancy disorder often complicated by reduced fetal growth or preterm delivery and is associated with long-term maternal morbidity and mortality. We aimed to assess the association between preeclampsia phenotypes and risk of subsequent coronary heart disease and maternal cardiovascular mortality.
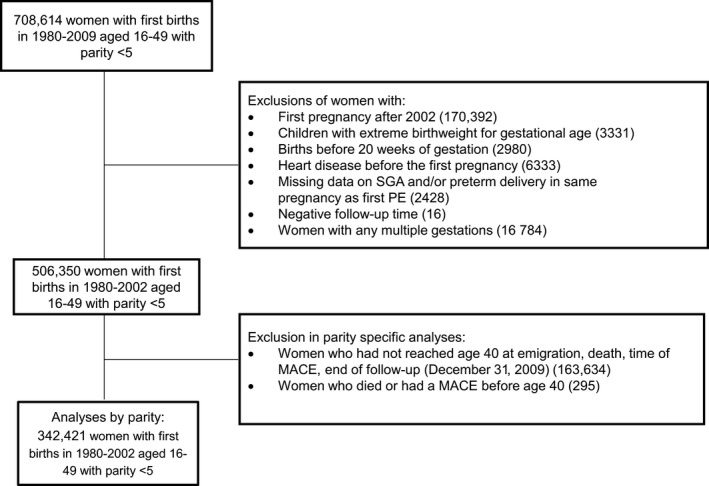
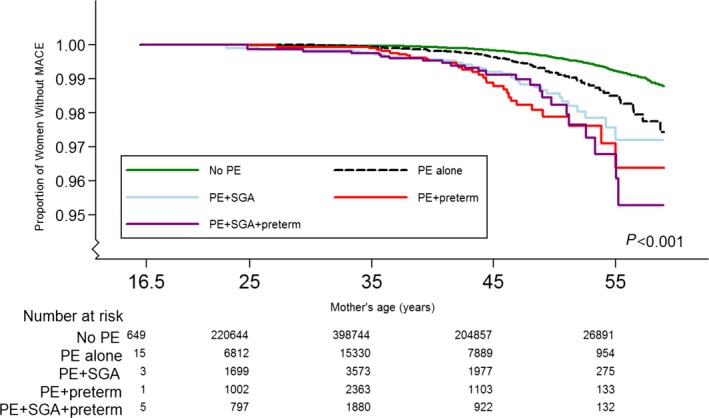
Methods and results: Women aged 16 to 49 years who gave birth during 1980-2002 and registered in the Medical Birth Registry of Norway were followed prospectively (1-29 years) for an incident major coronary event and mortality through linkage with the Cardiovascular Disease in Norway 1994-2009 (CVDNOR) project and the Norwegian Cause of Death Registry. Preeclampsia was subdivided based on the presence of a child born small for gestational age or preterm delivery. Among 506 350 women with 1 to 5 singleton births, there were 1275 (0.3%) occurrences of major coronary event, 468 (0.1%) cardiovascular deaths, and 5411 (1.1%) deaths overall. Compared with women without preeclampsia, the hazard ratio (95% CI) for major coronary event was 2.1 (1.73-2.65) after preeclampsia alone, 3.3 (2.37-4.57) after preeclampsia in combination with small for gestational age, and 5.4 (3.74-7.74) after preeclampsia in combination with preterm delivery. Analyses distinguishing women with 1 (n=61 352) or >1 (n=281 069) lifetime pregnancy and analyses with cardiovascular mortality as outcome followed the same pattern.
Conclusions: The occurrence of major coronary events was increased among women with preeclampsia and highest for preeclampsia combined with a child born small for gestational age and/or preterm delivery.
Keywords: cardiovascular disease; fetal growth restriction; major coronary events; preeclampsia; preterm delivery.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Redman CW, Sargent IL. Placental debris, oxidative stress and pre‐eclampsia. Placenta. 2000;21:597–602. - PubMed
-
- Odegard RA, Vatten LJ, Nilsen ST, Salvesen KA, Austgulen R. Risk factors and clinical manifestations of pre‐eclampsia. BJOG. 2000;107:1410–1416. - PubMed
-
- Staff AC, Dechend R, Redman CW. Review: preeclampsia, acute atherosis of the spiral arteries and future cardiovascular disease: two new hypotheses. Placenta. 2013;34(suppl):S73–S78. - PubMed
-
- Redman CW, Sargent IL. Placental stress and pre‐eclampsia: a revised view. Placenta. 2009;30(suppl A):S38–S42. - PubMed
-
- Chappell S, Morgan L. Searching for genetic clues to the causes of pre‐eclampsia. Clin Sci (Lond). 2006;110:443–458. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
