

Review
doi: 10.1161/HYPERTENSIONAHA.116.08956.
Arterial Hypertension, Atrial Fibrillation, and Hyperaldosteronism: The Triple Trouble
Affiliations
- PMID: 28264920
- PMCID: PMC5425097
- DOI: 10.1161/HYPERTENSIONAHA.116.08956
Item in Clipboard
Review
Arterial Hypertension, Atrial Fibrillation, and Hyperaldosteronism: The Triple Trouble
Hypertension.
2017 Apr.
No abstract available
Conflict of interest statement
Figures
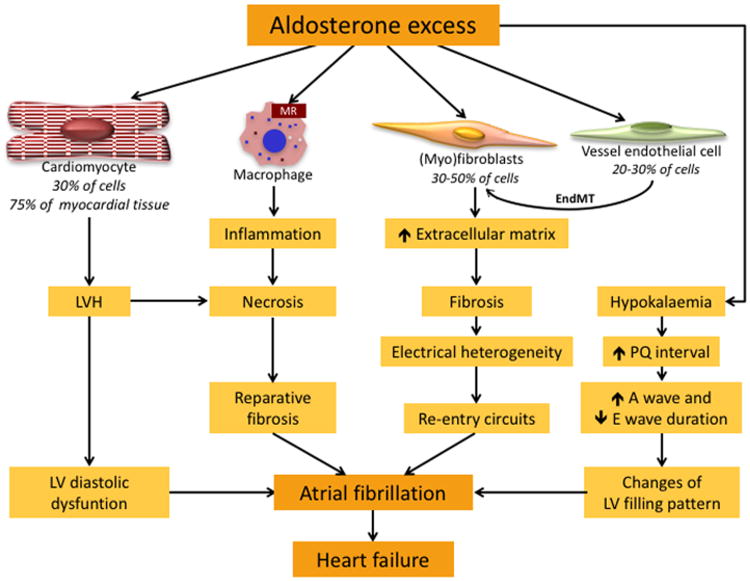
Aldosterone affects all cell types that are the primary constituents of cardiac tissue: a) cardiomyocytes, which constitute 30% of myocardial cells, but 75% of myocardial tissue, b) fibroblasts (30-50% of myocardial cells), c) endothelial cells (20-30% of myocardial cells), and also activates macrophages. Aldosterone excess induces enlargement of cardiomyocytes and remodeling leading to left ventricular hypertrophy (LVH) that predisposes to diastolic dysfunction. Aldosterone excess also activates the transition of fibroblasts into myofibroblasts, which produce collagen and other extracellular matrix proteins, favoring fibrosis. Fibrotic tissue induces electrical heterogeneity of the myocardium that causes re-entry circuits, thereby leading to onset of atrial fibrillation. Endothelial cells exposed to aldosterone excess undergo transition into myofibroblasts (endothelial-to-mesenchymal transition, EMT), which contribute to the development of fibrosis. The activation of the mineralocorticoid receptor (MR) on the monocytes/macrophages favors inflammation, necrosis and reparative fibrosis, and eventually atrial fibrillation. Aldosterone excess induces hypokalemia, which causes prolongation of PQ interval and changes in the duration of A and E waves, leading to abnormal LV filling that promotes AF, which in turn favors heart failure.
References
-
- Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37:2893–2962. - PubMed
-
- Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol. 2009;104:1534–1539. - PubMed
-
- Naccarelli GV, Johnston SS, Dalal M, Lin J, Patel PP. Rates and implications for hospitalization of patients >/=65 years of age with atrial fibrillation/flutter. Am J Cardiol. 2012;109:543–549. - PubMed
-
- Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 1998;82:2N–9N. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
