

Multisensor-integrated organs-on-chips platform for automated and continual in situ monitoring of organoid behaviors
- PMID: 28265064
- PMCID: PMC5373350
- DOI: 10.1073/pnas.1612906114
Multisensor-integrated organs-on-chips platform for automated and continual in situ monitoring of organoid behaviors
Abstract
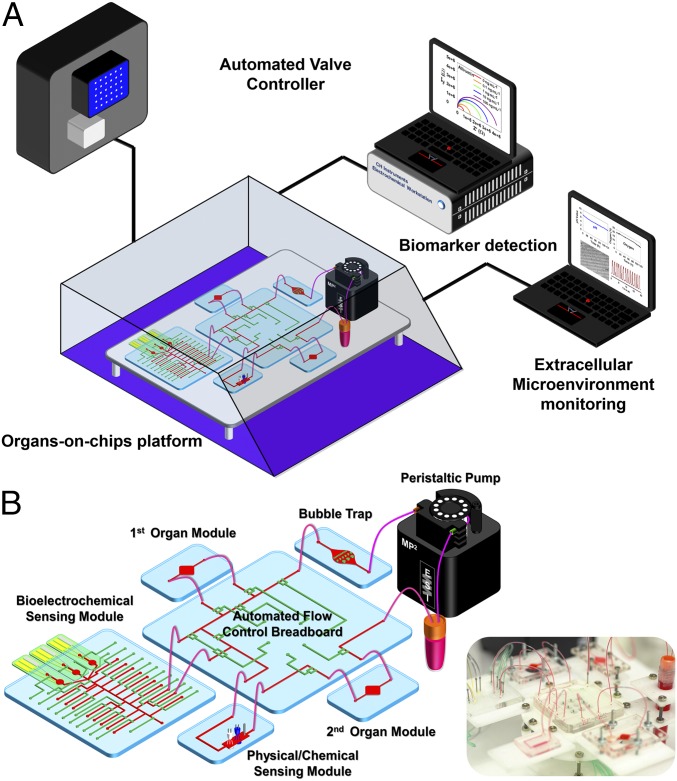
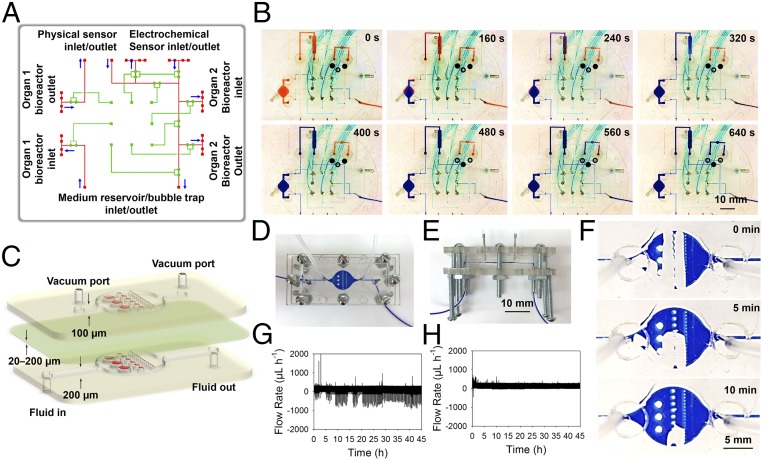
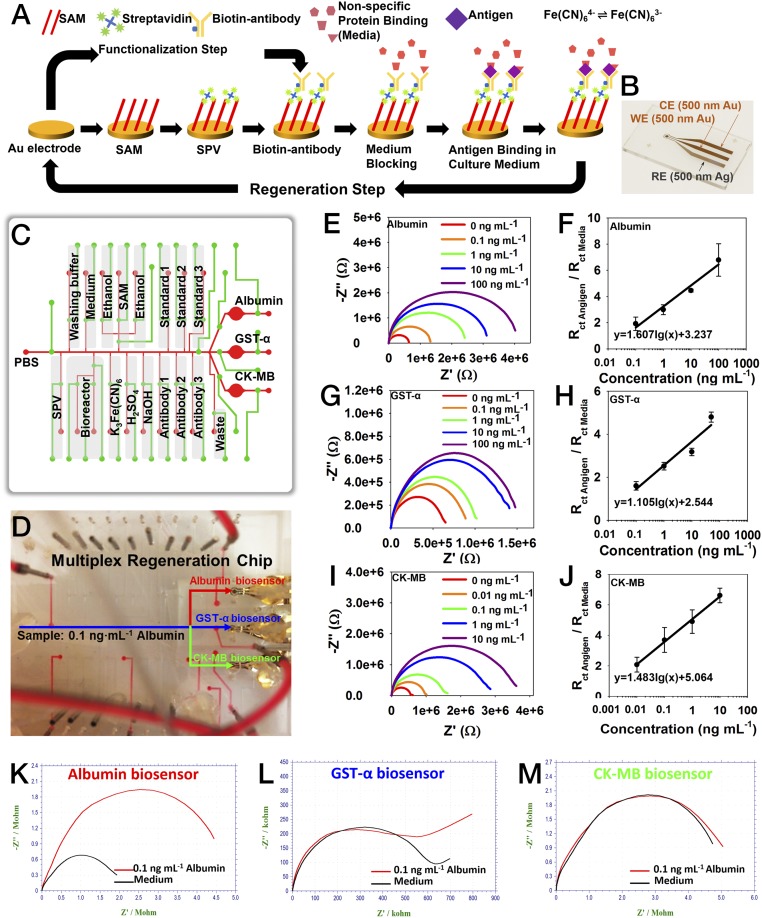
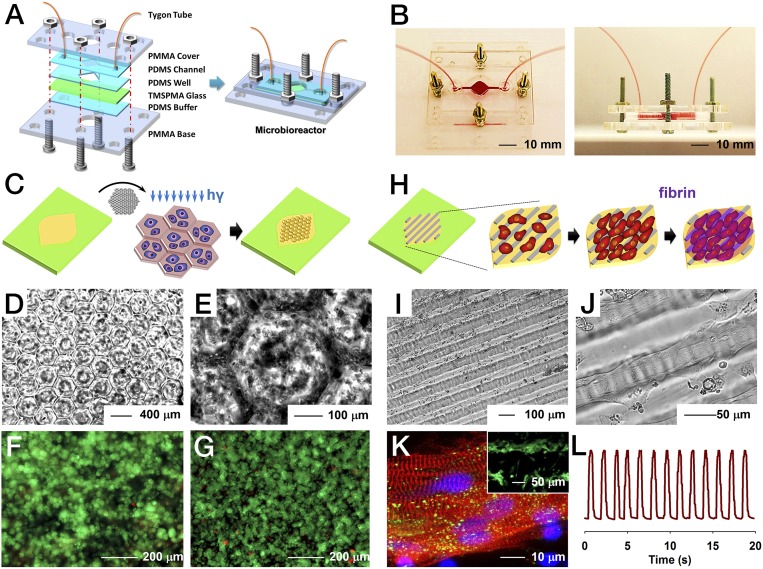
Organ-on-a-chip systems are miniaturized microfluidic 3D human tissue and organ models designed to recapitulate the important biological and physiological parameters of their in vivo counterparts. They have recently emerged as a viable platform for personalized medicine and drug screening. These in vitro models, featuring biomimetic compositions, architectures, and functions, are expected to replace the conventional planar, static cell cultures and bridge the gap between the currently used preclinical animal models and the human body. Multiple organoid models may be further connected together through the microfluidics in a similar manner in which they are arranged in vivo, providing the capability to analyze multiorgan interactions. Although a wide variety of human organ-on-a-chip models have been created, there are limited efforts on the integration of multisensor systems. However, in situ continual measuring is critical in precise assessment of the microenvironment parameters and the dynamic responses of the organs to pharmaceutical compounds over extended periods of time. In addition, automated and noninvasive capability is strongly desired for long-term monitoring. Here, we report a fully integrated modular physical, biochemical, and optical sensing platform through a fluidics-routing breadboard, which operates organ-on-a-chip units in a continual, dynamic, and automated manner. We believe that this platform technology has paved a potential avenue to promote the performance of current organ-on-a-chip models in drug screening by integrating a multitude of real-time sensors to achieve automated in situ monitoring of biophysical and biochemical parameters.
Keywords: drug screening; electrochemical biosensor; microbioreactor; organ-on-a-chip; physical sensor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Paul SM, et al. How to improve R&D productivity: The pharmaceutical industry’s grand challenge. Nat Rev Drug Discov. 2010;9(3):203–214. - PubMed
-
- US Food and Drug Administration 2015 Drug-Induced Liver Toxicity. Available at www.fda.gov/Drugs/ScienceResearch/ResearchAreas/ucm071471.htm. Accessed March 30, 2016.
-
- Hay M, Thomas DW, Craighead JL, Economides C, Rosenthal J. Clinical development success rates for investigational drugs. Nat Biotechnol. 2014;32(1):40–51. - PubMed
-
- Arrowsmith J, Miller P. Trial watch: Phase II and phase III attrition rates 2011–2012. Nat Rev Drug Discov. 2013;12(8):569. - PubMed
-
- Ferri N, et al. Drug attrition during pre-clinical and clinical development: Understanding and managing drug-induced cardiotoxicity. Pharmacol Ther. 2013;138(3):470–484. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
