

PET/CT imaging in polymyalgia rheumatica: praepubic 18F-FDG uptake correlates with pectineus and adductor longus muscles enthesitis and with tenosynovitis
- PMID: 28265227
- PMCID: PMC5330169
- DOI: 10.1515/raon-2017-0001
PET/CT imaging in polymyalgia rheumatica: praepubic 18F-FDG uptake correlates with pectineus and adductor longus muscles enthesitis and with tenosynovitis
Abstract
Background: The role of 18F-fluorodeoxyglucose positron emission computed tomography (18F-FDG PET/CT) is increasing in the diagnosis of polymyalgia rheumatica (PMR), one of the most common inflammatory rheumatic diseases. In addition to other locations, increased 18F-FDG accumulation has been detected in the praepubic region in some patients. However, a deeper description and pathophysiological explanation of this increased praepubic accumulation has been lacking. The aim of the presented study is to confirm a decrease in praepubic 18F-FDG accumulation in response to therapy and to describe potential correlations to other 18F-FDG PET/CT scan characteristics during the course of disease. As a secondary objective, we describe the pathological aspects of the observed praepubic 18F-FDG uptake.
Patients and methods: A retrospective review of patients with newly suspected PMR undergoing baseline and follow up 18F-FDG PET/CT between February 2010 and March 2016 is given. Those with a visually detected presence of praepubic 18F-FDG accumulation were further analysed. The uptake was assessed visually and also semi-quantitatively in the defined region of interest by calculation of target-to-liver ratios. Other regions typical for PMR were systematically described as well (shoulders, hips, sternoclavicular joints, ischiogluteal bursae, spinous interspaces).
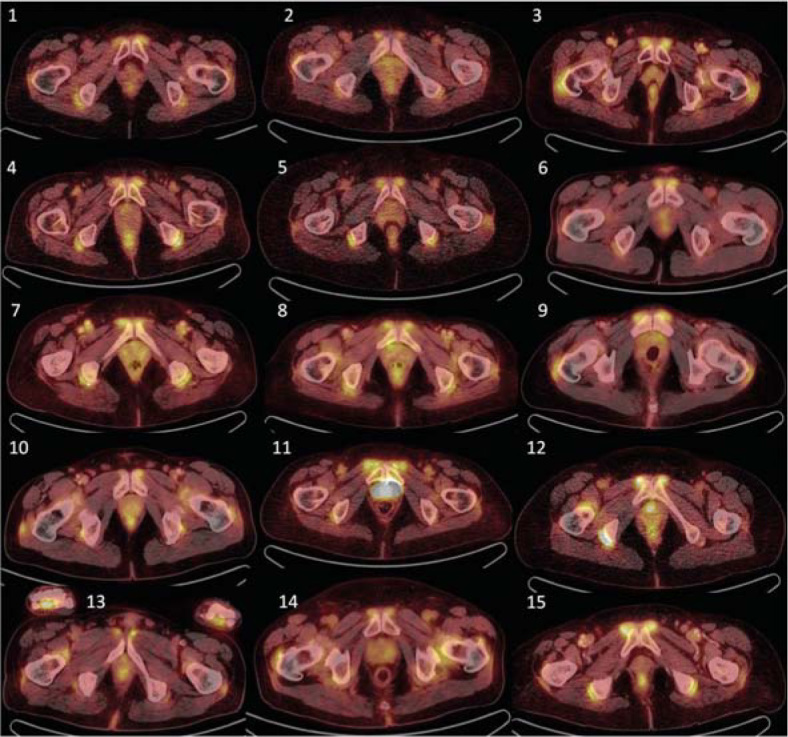
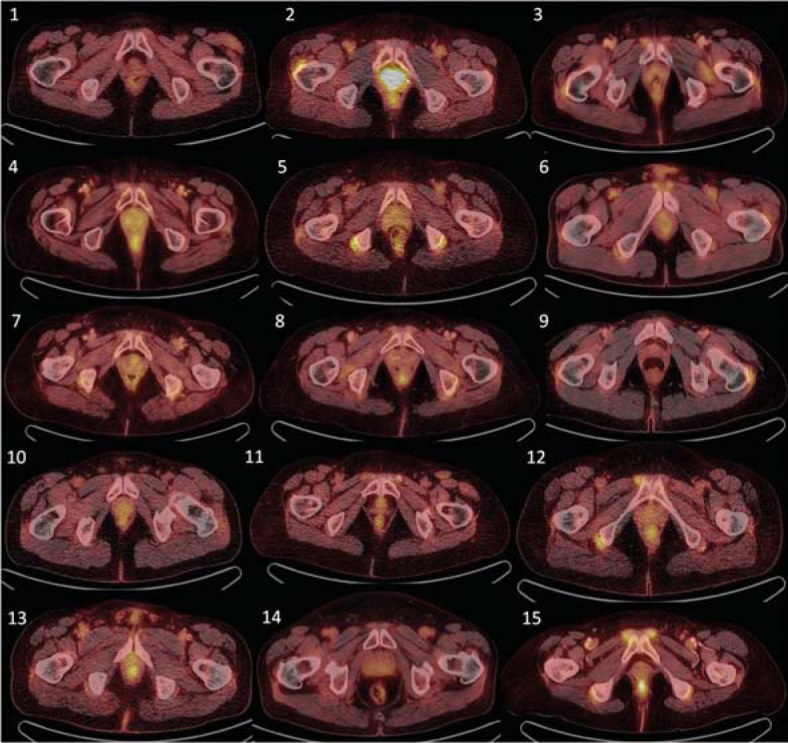
Results: Twenty-three out of 89 screened patients (26%) presented with initial praepubic 18F-FDG PET/CT positivity, 15 of whom also underwent follow up 18F-FDG PET/CT examination. Five out of 15 patients presented with increased 18F-FDG accumulation in large arteries as a sign of giant cell arteritis. During follow up examination, decrease in 18F-FDG accumulation caused by therapeutic intervention was observed in all evaluated locations in all analysed patients and no new positivity was indicated, including periarticular, extraarticular tissues or target large vessels. Praepubical accumulation of 18F-FDG was diminished in all patients (15/15, 100%) after treatment with steroids.
Conclusions: Increased praepubic 18F-FDG uptake in patients with PMR is relatively common and this region should be systematically evaluated during differential diagnosis of rheumatic and malignant disease. Praepubic inflammation is probably related to enthesitis and tenosynovitis at the origin of pectineus and adductor longus muscles ventrally from the pubis.
Keywords: enthesitis; fluorodeoxyglucose; polymyalgia rheumatica; positron emission tomography; tenosynovitis.
Figures
Similar articles
-
Diagnostic value of [18F]FDG-PET/CT in polymyalgia rheumatica: a systematic review and meta-analysis.Eur J Nucl Med Mol Imaging. 2021 Jun;48(6):1876-1889. doi: 10.1007/s00259-020-05162-6. Epub 2020 Dec 28. Eur J Nucl Med Mol Imaging. 2021. PMID: 33372248 Free PMC article.
-
18F-FDG PET/CT in polymyalgia rheumatica-a pictorial review.Br J Radiol. 2017 Aug;90(1076):20170198. doi: 10.1259/bjr.20170198. Epub 2017 Jun 16. Br J Radiol. 2017. PMID: 28508663 Free PMC article. Review.
-
Various forms of (18)F-FDG PET and PET/CT findings in patients with polymyalgia rheumatica.Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015 Dec;159(4):629-36. doi: 10.5507/bp.2015.026. Epub 2015 May 25. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015. PMID: 26006092
-
Diagnosing polymyalgia rheumatica on 18F-FDG PET/CT: typical uptake patterns.Ann Nucl Med. 2018 Oct;32(8):573-577. doi: 10.1007/s12149-018-1269-5. Epub 2018 Jun 8. Ann Nucl Med. 2018. PMID: 29948622
-
Differentiation between Polymyalgia Rheumatica (PMR) and Elderly-Onset Rheumatoid Arthritis Using 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography: Is Enthesitis a New Pathological Lesion in PMR?PLoS One. 2016 Jul 6;11(7):e0158509. doi: 10.1371/journal.pone.0158509. eCollection 2016. PLoS One. 2016. PMID: 27384410 Free PMC article.
Cited by
-
MRI of shoulder girdle in polymyalgia rheumatica: inflammatory findings and their diagnostic value.RMD Open. 2024 May 9;10(2):e004169. doi: 10.1136/rmdopen-2024-004169. RMD Open. 2024. PMID: 38724260 Free PMC article.
-
Diagnostic value of [18F]FDG-PET/CT in polymyalgia rheumatica: a systematic review and meta-analysis.Eur J Nucl Med Mol Imaging. 2021 Jun;48(6):1876-1889. doi: 10.1007/s00259-020-05162-6. Epub 2020 Dec 28. Eur J Nucl Med Mol Imaging. 2021. PMID: 33372248 Free PMC article.
-
Characterising polymyalgia rheumatica on whole-body 18F-FDG PET/CT: an atlas.Rheumatol Adv Pract. 2024 Feb 20;8(1):rkae003. doi: 10.1093/rap/rkae003. eCollection 2024. Rheumatol Adv Pract. 2024. PMID: 38375531 Free PMC article. Review.
-
18F-FDG PET/CT in polymyalgia rheumatica-a pictorial review.Br J Radiol. 2017 Aug;90(1076):20170198. doi: 10.1259/bjr.20170198. Epub 2017 Jun 16. Br J Radiol. 2017. PMID: 28508663 Free PMC article. Review.
-
Disease stratification in GCA and PMR: state of the art and future perspectives.Nat Rev Rheumatol. 2023 Jul;19(7):446-459. doi: 10.1038/s41584-023-00976-8. Epub 2023 Jun 12. Nat Rev Rheumatol. 2023. PMID: 37308659 Review.
References
-
- Nesjet G,, Nesjet R. In: Vasculitis (2nd ed.) Ball GV,, Bridges SL Jr, editors. Oxford University Press; 2008. Giant cell arteritis and polymyalgia rheumatica; pp. 307–16.
-
- Cantini F,, Nicoli L,, Nannini C,, Padula A,, Olivieri I,, Boiardi L,. et al. Inflammatory changes of the hip synovial structures in polymyalgia rheumatica. Clin Exp Rheumatol. 2005;23:462–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials