

Diagnosing the frontal variant of Alzheimer's disease: a clinician's yellow brick road
- PMID: 28265458
- PMCID: PMC5333400
- DOI: 10.1186/s40734-017-0052-4
Diagnosing the frontal variant of Alzheimer's disease: a clinician's yellow brick road
Abstract
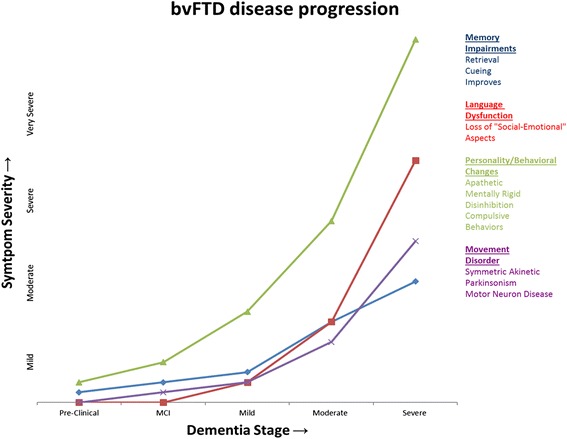
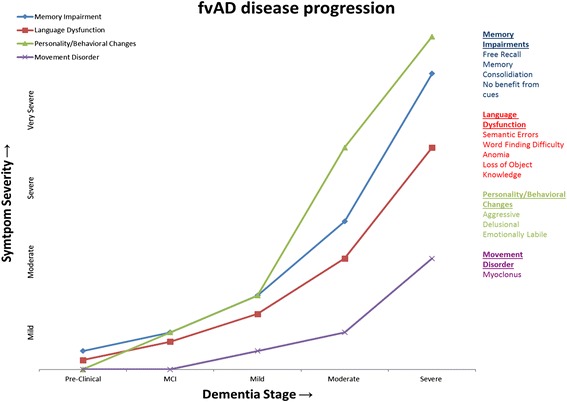
Background: Disruption of the frontal lobes and its associated networks are a common consequence of neurodegenerative disorders. Given the wide range of cognitive, behavioral and motor processes in which the frontal lobes are involved, there can be a great variety of manifestations depending on the pathology distribution. The most common are the behavioral variant of frontotemporal dementia (bvFTD) and the frontal variant of Alzheimer's disease (fvAD), which are particularly challenging to disentangle. Recognizing fvAD from bvFTD-related pathologies is a diagnostic challenge and a critical need in the management and counseling of these patients.
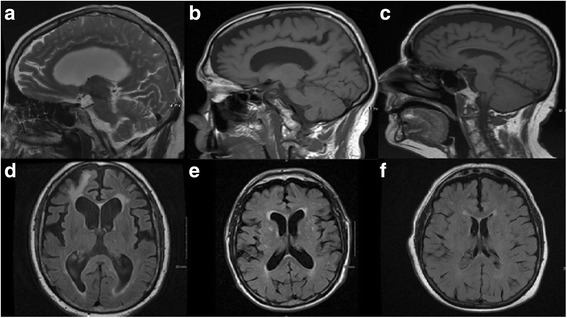
Case presentation: Here we present three pathology-proven cases of Alzheimer's disease initially misdiagnosed as bvFTD and discuss the distinctive or less overlapping historical, examination, and laboratory findings of fvAD and bvFTD, deriving analogies for mnemonic endurance from the Wizard of Oz worldview.
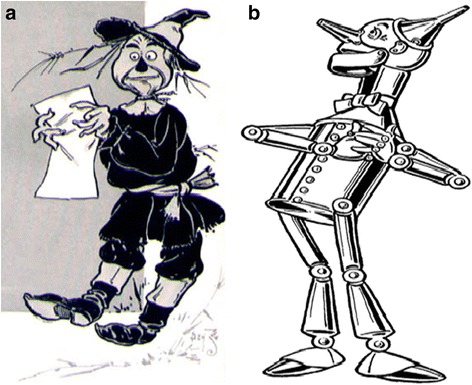
Conclusion: The Yellow Brick Road to diagnosing these disorders may be served by the metaphor of fvAD as the irritable, paranoid, and tremulous Scarecrow and bvFTD the heartless, ritualistic, and rigid Tin Man. An Oz-inspired creative license may help the clinician recognize the differential disease progression, caregiver burden, and treatment response of fvAD compared with bvFTD.
Keywords: Behavioral disorder; Frontal variant of Alzheimer’s disease; Frontotemporal Dementia; Movement disorders; Parkinsonism.
Figures
References
-
- Hyman BT, Phelps CH, Beach TG, Bigio EH, Cairns NJ, Carrillo MC, Dickson DW, Duyckaerts C, Frosch MP, Masliah E, et al. National Institute on Aging-Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease. Alzheimers Dement. 2012;8:1–13. doi: 10.1016/j.jalz.2011.10.007. - DOI - PMC - PubMed
-
- Mirra SS, Heyman A, McKeel D, Sumi SM, Crain BJ, Brownlee LM, Vogel FS, Hughes JP, Van Belle G, Berg L. The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part II. Standardization of the neuropathologic assessment of Alzheimer’s disease. Neurology. 1991;41:479–486. doi: 10.1212/WNL.41.4.479. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
