

Longitudinal Impact of the Smoking Ban Legislation in Acute Coronary Syndrome Admissions
- PMID: 28265574
- PMCID: PMC5318631
- DOI: 10.1155/2017/6956941
Longitudinal Impact of the Smoking Ban Legislation in Acute Coronary Syndrome Admissions
Abstract
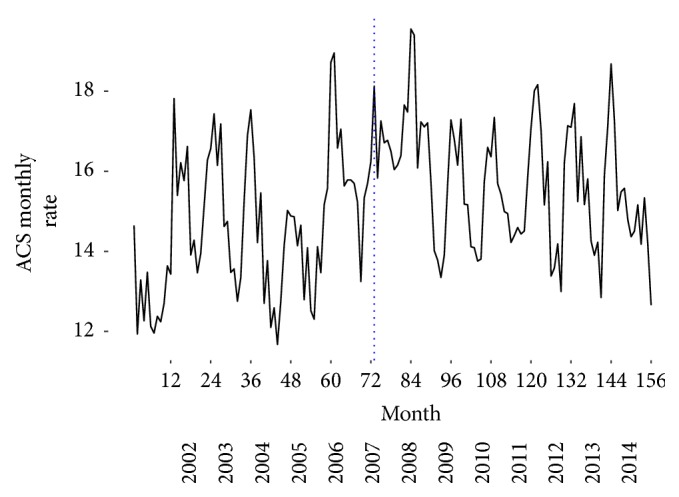
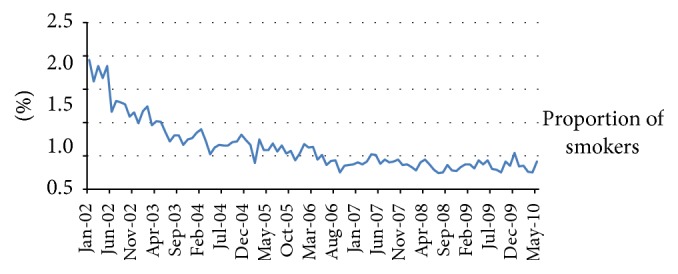
Background and Purpose. The association between smoking and CV has been proved; however smoking is still the first preventable cause of death in the EU. We aim to evaluate the potential impact of the smoke ban on the number of ACS events in the Portuguese population. In addition, we evaluate the longitudinal effects of the smoking ban several years after its implementation. Methods. We analyzed the admission rate for ACS before and after the ban using data from hospital admission. Monthly crude rate was computed, using the Portuguese population as the denominator. Data concerning the proportion of smokers among ACS patients were obtained from the NRACS. Interrupted time series were used to assess changes over time. Results. A decline of -5.8% was found for ACS crude rate after the smoking ban. The decreasing trend was observed even after years since the law. The effect of the ban was higher in men and for people over 65 years. The most significant reduction of ACS rate was found in Lisbon. Conclusions. Our results suggest that smoking ban is related to a decline in ACS admissions, supporting the importance of smoke legislation as a public health measure, contributing to the reduction of ACS rate.
Conflict of interest statement
The authors declare that there is no conflict of interests regarding the publication of this paper.
Figures
Similar articles
-
Changes in hospitalization rates for acute coronary syndrome after a two-phase comprehensive smoking ban.Eur J Prev Cardiol. 2014 Dec;21(12):1575-82. doi: 10.1177/2047487313500569. Epub 2013 Aug 5. Eur J Prev Cardiol. 2014. PMID: 23918841
-
Impact of a national smoking ban on hospital admission for acute coronary syndromes: a longitudinal study.Clin Cardiol. 2012 Apr;35(4):205-9. doi: 10.1002/clc.21014. Epub 2012 Jan 25. Clin Cardiol. 2012. PMID: 22278857 Free PMC article.
-
Design of prospective study of acute coronary syndrome hospitalization after smoking ban in public places in Hyogo prefecture: comparison with Gifu, a prefecture without a public smoking ban.J Cardiol. 2014 Feb;63(2):165-8. doi: 10.1016/j.jjcc.2013.06.020. Epub 2013 Aug 22. J Cardiol. 2014. PMID: 23972686
-
Acute pulmonary admissions following implementation of a national workplace smoking ban.Chest. 2012 Sep;142(3):673-679. doi: 10.1378/chest.11-2757. Chest. 2012. PMID: 22383660
-
The impact of public smoking ban on the incidence of myocardial infarction hospitalizations.Rev Cardiovasc Med. 2010 Summer;11(3):e121-9. doi: 10.3909/ricm0540. Rev Cardiovasc Med. 2010. PMID: 21045764 Review.
Cited by
-
Adult vaccination as part of a healthy lifestyle: moving from medical intervention to health promotion.Ann Med. 2019 Mar;51(2):128-140. doi: 10.1080/07853890.2019.1588470. Epub 2019 Apr 26. Ann Med. 2019. PMID: 31025882 Free PMC article. Review.
-
Prevalence of Acute Myocardial Infarction and Changing Meteorological Conditions in Iran: Fuzzy Clustering Approach.Iran J Public Health. 2020 May;49(5):923-930. Iran J Public Health. 2020. PMID: 32953680 Free PMC article.
-
Trends of case-fatality rate by acute coronary syndrome in Portugal: Impact of a fast track to the coronary unit.JRSM Cardiovasc Dis. 2019 May 24;8:2048004019851952. doi: 10.1177/2048004019851952. eCollection 2019 Jan-Dec. JRSM Cardiovasc Dis. 2019. PMID: 31205687 Free PMC article.
-
Evaluation of Population-Level Tobacco Control Interventions and Health Outcomes: A Systematic Review and Meta-Analysis.JAMA Netw Open. 2023 Jul 3;6(7):e2322341. doi: 10.1001/jamanetworkopen.2023.22341. JAMA Netw Open. 2023. PMID: 37418258 Free PMC article.
-
Smoke-free hospitality environments and cognitive health: A population-based study in the United States.Prev Med Rep. 2025 Jan 3;50:102961. doi: 10.1016/j.pmedr.2024.102961. eCollection 2025 Feb. Prev Med Rep. 2025. PMID: 39877081 Free PMC article.
References
-
- Scoggins A., de Vries H., Conklin A., Hatziandreu E. Analysis to Support the Impact Assessment of the Commission's Smoke-Free Initiatives. Santa Monica, Calif, USA: RAND; 2009.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
