

The Role of a Hospital Ethics Consultation Service in Decision-Making for Unrepresented Patients
- PMID: 28265798
- PMCID: PMC5529225
- DOI: 10.1007/s11673-017-9773-1
The Role of a Hospital Ethics Consultation Service in Decision-Making for Unrepresented Patients
Abstract
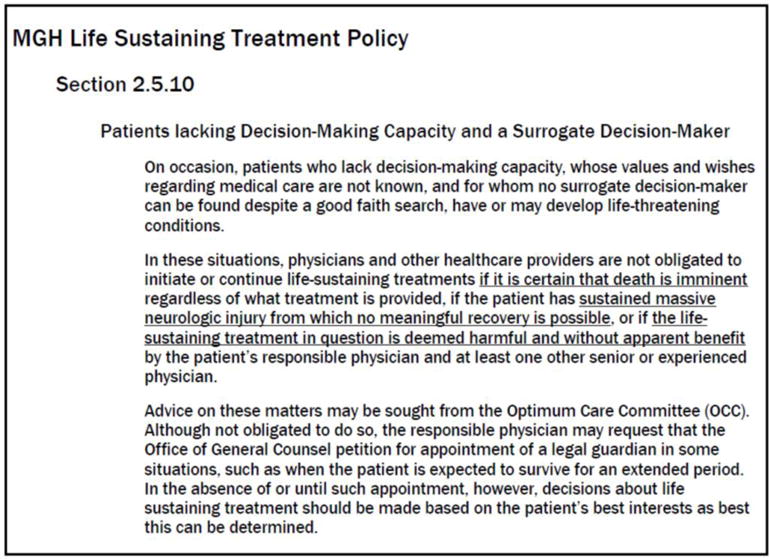
Despite increased calls for hospital ethics committees to serve as default decision-makers about life-sustaining treatment (LST) for unrepresented patients who lack decision-making capacity or a surrogate decision-maker and whose wishes regarding medical care are not known, little is known about how committees currently function in these cases. This was a retrospective cohort study of all ethics committee consultations involving decision-making about LST for unrepresented patients at a large academic hospital from 2007 to 2013. There were 310 ethics committee consultations, twenty-five (8.1 per cent) of which involved unrepresented patients. In thirteen (52.0 per cent) cases, the ethics consultants evaluated a possible substitute decision-maker identified by social workers and/or case managers. In the remaining cases, the ethics consultants worked with the medical team to contact previous healthcare professionals to provide substituted judgement, found prior advance care planning documents, or identified the patient's best interest as the decision-making standard. In the majority of cases, the final decision was to limit or withdraw LST (72 per cent) or to change code status to Do Not Resuscitate/Do Not Intubate (12 per cent). Substitute decision-makers who had been evaluated through the ethics consultation process and who made the final decision alone were more likely to continue LST than cases in which physicians made the final decision (50 per cent vs 6.3 per cent, p = 0.04). In our centre, the primary role of ethics consultants in decision-making for unrepresented patients is to identify appropriate decision-making standards. In the absence of other data suggesting that ethics committees, as currently constituted, are ready to serve as substitute decision-makers for unrepresented patients, caution is necessary before designating these committees as default decision-makers.
Keywords: Best interests; Decision-making; Ethics committees; Ethics consultation; Surrogates; Unrepresented.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Who should Decide for the Unrepresented?Bioethics. 2016 Mar;30(3):173-80. doi: 10.1111/bioe.12185. Epub 2015 Aug 26. Bioethics. 2016. PMID: 26307414
-
Making Medical Treatment Decisions for Unrepresented Patients in the ICU. An Official American Thoracic Society/American Geriatrics Society Policy Statement.Am J Respir Crit Care Med. 2020 May 15;201(10):1182-1192. doi: 10.1164/rccm.202003-0512ST. Am J Respir Crit Care Med. 2020. PMID: 32412853 Free PMC article.
-
Care of Patients at the End of Life: Surrogate Decision Making for Incapacitated Patients.FP Essent. 2016 Aug;447:32-41. FP Essent. 2016. PMID: 27490071
-
The effect of statutory limitations on the authority of substitute decision makers on the care of patients in the intensive care unit: case examples and review of state laws affecting withdrawing or withholding life-sustaining treatment.J Intensive Care Med. 2014 Mar-Apr;29(2):71-80. doi: 10.1177/0885066611433551. Epub 2012 Jan 17. J Intensive Care Med. 2014. PMID: 22257784 Review.
-
Deciding for others.Milbank Q. 1986;64(Suppl. 2):17-94. Milbank Q. 1986. PMID: 11649884 Review.
Cited by
-
Sex, Drugs, and a Few Other Things.J Bioeth Inq. 2017 Jun;14(2):163-165. doi: 10.1007/s11673-017-9786-9. J Bioeth Inq. 2017. PMID: 28608055 No abstract available.
-
The Role of Healthcare Chaplains in Resuscitation: A Rapid Literature Review.J Relig Health. 2018 Jun;57(3):1183-1195. doi: 10.1007/s10943-018-0604-4. J Relig Health. 2018. PMID: 29569111 Review.
-
Making Medical Decisions for Incapacitated Patients Without Proxies: Part II.HEC Forum. 2020 Mar;32(1):47-62. doi: 10.1007/s10730-019-09388-2. HEC Forum. 2020. PMID: 31691879 Free PMC article.
-
Making Medical Decisions for Incapacitated Patients Without Proxies: Part I.HEC Forum. 2020 Mar;32(1):33-45. doi: 10.1007/s10730-019-09387-3. HEC Forum. 2020. PMID: 31686275
-
Caring for Unbefriended Older Adults and Adult Orphans: A Clinician Survey.Clin Gerontol. 2021 Jul-Sep;44(4):494-503. doi: 10.1080/07317115.2019.1640332. Epub 2019 Jul 15. Clin Gerontol. 2021. PMID: 31305222 Free PMC article.
References
-
- American Bar Association. Default surrogate consents statutes as of June 2014. 2014 Available at: http://www.americanbar.org/content/dam/aba/administrative/law_aging/2014.... Accessed November 17, 2015.
-
- Brock D. Death and dying: Euthanasia and sustaining life: Ethical issues. In: Reich E, editor. Encyclopedia of Bioethics. New York: Simon and Schuster; 1995. pp. 563–572.
-
- Courtwright AM, Brackett S, Cadge W, Krakauer EK, Robinson EM. Experience with a hospital policy on not offering cardiopulmonary resuscitation when believed more harmful than beneficial. Journal of Critical Care. 2015;30(1):173–177. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
