

Coronary Artery Disease in HIV-Infected Patients: Downside of Living Longer
- PMID: 28265887
- PMCID: PMC6066371
- DOI: 10.1007/s11883-017-0651-4
Coronary Artery Disease in HIV-Infected Patients: Downside of Living Longer
Abstract
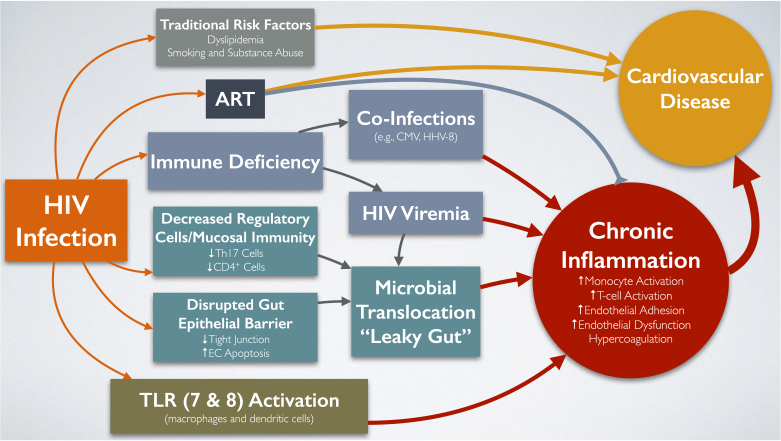
Purpose of review: Introduction of combination antiretroviral therapy (ART) has increased the life expectancy of patients with HIV infection, allowing them to live longer with this chronic medical condition and consequently experiencing conditions such as cardiovascular diseases (CVDs). Several studies have investigated the increased risk of CVD in people living with HIV (PLWH). However, less is known about the exact mechanisms involved in this increased risk. Also, specific guidelines for management of CVD in PLWH have not been developed yet. In this article, we review the recent literature on the mechanisms involved in pathogenesis of CVD in PLWH, with an emphasis on coronary artery disease (CAD).
Recent findings: Although initial studies suspected the increased prevalence of traditional CVD risk factors and side effects of ART to be involved in the increased CVD risk in PLWH, recent studies have uncovered the important role of chronic persistent inflammation in this increased risk. In addition, biomarkers of inflammation have been associated with both CVD events and subclinical CAD in this population. Lastly, recent studies and ongoing clinical trials have been investigating medical interventions that aim to reduce inflammation and cardiovascular events. Different mechanisms of inflammation have been examined in PLWH, including subclinical viremia, microbial translocation, and coinfection with other pathogens such as cytomegalovirus. Although inflammatory biomarkers have been consistently associated with CVD and subclinical CVD outcomes, their prognostic value is unknown. Recent and ongoing trials are exploring the benefits of anti-inflammatory drugs, statins, and antimicrobial translocation drugs on both inflammation and CVD risk among PLWH.
Keywords: Biomarkers; Cardiovascular disease; Clinical trials; Coronary artery disease; HIV infection; Inflammation.
Conflict of interest statement
Figures
Similar articles
-
HIV Infection and Risk of Cardiovascular Diseases Beyond Coronary Artery Disease.Curr Atheroscler Rep. 2017 May;19(5):20. doi: 10.1007/s11883-017-0652-3. Curr Atheroscler Rep. 2017. PMID: 28315199 Free PMC article. Review.
-
How Monocytes Contribute to Increased Risk of Atherosclerosis in Virologically-Suppressed HIV-Positive Individuals Receiving Combination Antiretroviral Therapy.Front Immunol. 2019 Jun 19;10:1378. doi: 10.3389/fimmu.2019.01378. eCollection 2019. Front Immunol. 2019. PMID: 31275317 Free PMC article. Review.
-
Higher cardiovascular disease risks in people living with HIV: A systematic review and meta-analysis.J Glob Health. 2024 Apr 26;14:04078. doi: 10.7189/jogh.14.04078. J Glob Health. 2024. PMID: 38666515 Free PMC article.
-
Cardiovascular disease in HIV patients: recent advances in predicting and managing risk.Expert Rev Anti Infect Ther. 2020 Jul;18(7):677-688. doi: 10.1080/14787210.2020.1757430. Epub 2020 May 20. Expert Rev Anti Infect Ther. 2020. PMID: 32306781 Review.
-
Upregulated IL-32 Expression And Reduced Gut Short Chain Fatty Acid Caproic Acid in People Living With HIV With Subclinical Atherosclerosis.Front Immunol. 2021 Apr 15;12:664371. doi: 10.3389/fimmu.2021.664371. eCollection 2021. Front Immunol. 2021. PMID: 33936102 Free PMC article.
Cited by
-
Coronary Microvascular Dysfunction in HIV: A Review.J Am Heart Assoc. 2020 Jan 7;9(1):e014018. doi: 10.1161/JAHA.119.014018. Epub 2019 Dec 19. J Am Heart Assoc. 2020. PMID: 31852423 Free PMC article. Review. No abstract available.
-
Vascular cognitive impairment and HIV-associated neurocognitive disorder: a new paradigm.J Neurovirol. 2019 Oct;25(5):710-721. doi: 10.1007/s13365-018-0706-5. Epub 2019 Jan 11. J Neurovirol. 2019. PMID: 30635846 Review.
-
Mapping strategies, components, and theories used in health education and physical activity interventions to prevent cardiovascular diseases in adults living with HIV: A scoping review protocol.PLoS One. 2025 Aug 1;20(8):e0312969. doi: 10.1371/journal.pone.0312969. eCollection 2025. PLoS One. 2025. PMID: 40748914 Free PMC article.
-
Role of Brain Arterial Remodeling in HIV-Associated Cerebrovascular Outcomes.Front Neurol. 2021 Jun 22;12:593605. doi: 10.3389/fneur.2021.593605. eCollection 2021. Front Neurol. 2021. PMID: 34239489 Free PMC article. Review.
-
mTOR regulation of metabolism limits LPS-induced monocyte inflammatory and procoagulant responses.Commun Biol. 2022 Aug 26;5(1):878. doi: 10.1038/s42003-022-03804-z. Commun Biol. 2022. PMID: 36028574 Free PMC article.
References
-
- Global Health Observatory data on HIV/AIDS [http://www.who. int/gho/hiv/en/]
-
- Vella S, Schwartlander B, Sow SP, Eholie SP, Murphy RL: The history of antiretroviral therapy and of its implementation in resource-limited areas of the world. AIDS (London, England) 2012, 26(10): 1231–1241. - PubMed
-
- Ho JE, Hsue PY. Cardiovascular manifestations of HIV infection. Heart. 2009;95(14):1193–202. - PubMed
-
- Farahani M, Mulinder H, Farahani A, Marlink R: Prevalence and distribution of non-AIDS causes of death among HIV-infected individuals receiving antiretroviral therapy: a systematic review and meta-analysis. Int J STD AIDS 2016. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
