

Multimorbidity and the risk of hospitalization and death in atrial fibrillation: A population-based study
- PMID: 28267478
- PMCID: PMC5343767
- DOI: 10.1016/j.ahj.2016.11.008
Multimorbidity and the risk of hospitalization and death in atrial fibrillation: A population-based study
Abstract
Patients with atrial fibrillation (AF) have many comorbidities and excess risks of hospitalization and death. Whether the impact of comorbidities on outcomes is greater in AF than the general population is unknown.
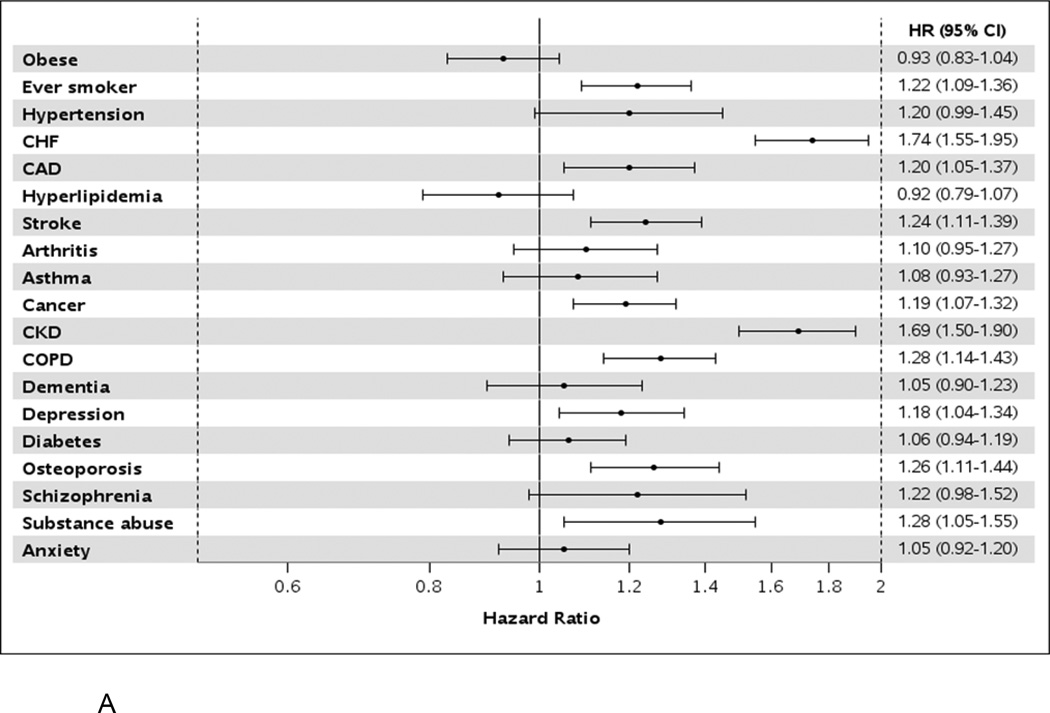
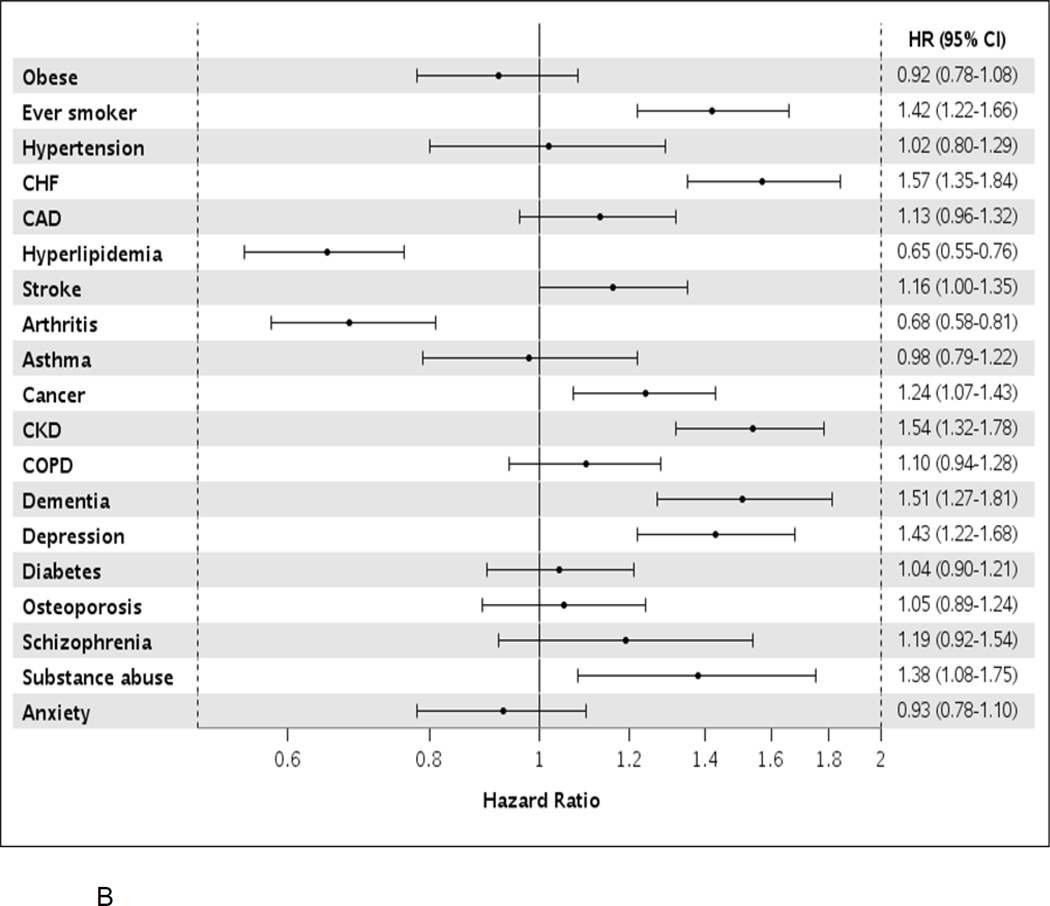
Methods: One thousand four hundred thirty patients with AF and community controls matched 1:1 on age and sex were obtained from Olmsted County, Minnesota. Andersen-Gill and Cox regression estimated associations of 19 comorbidities with hospitalization and death, respectively.
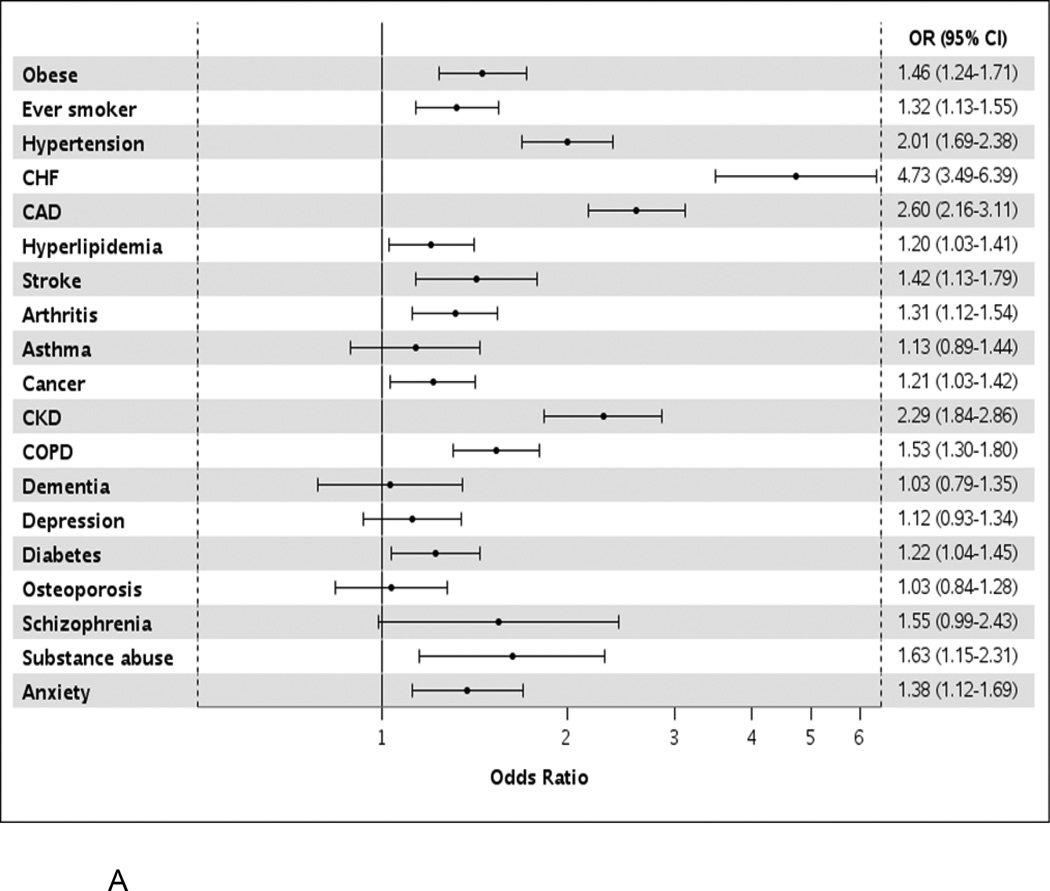
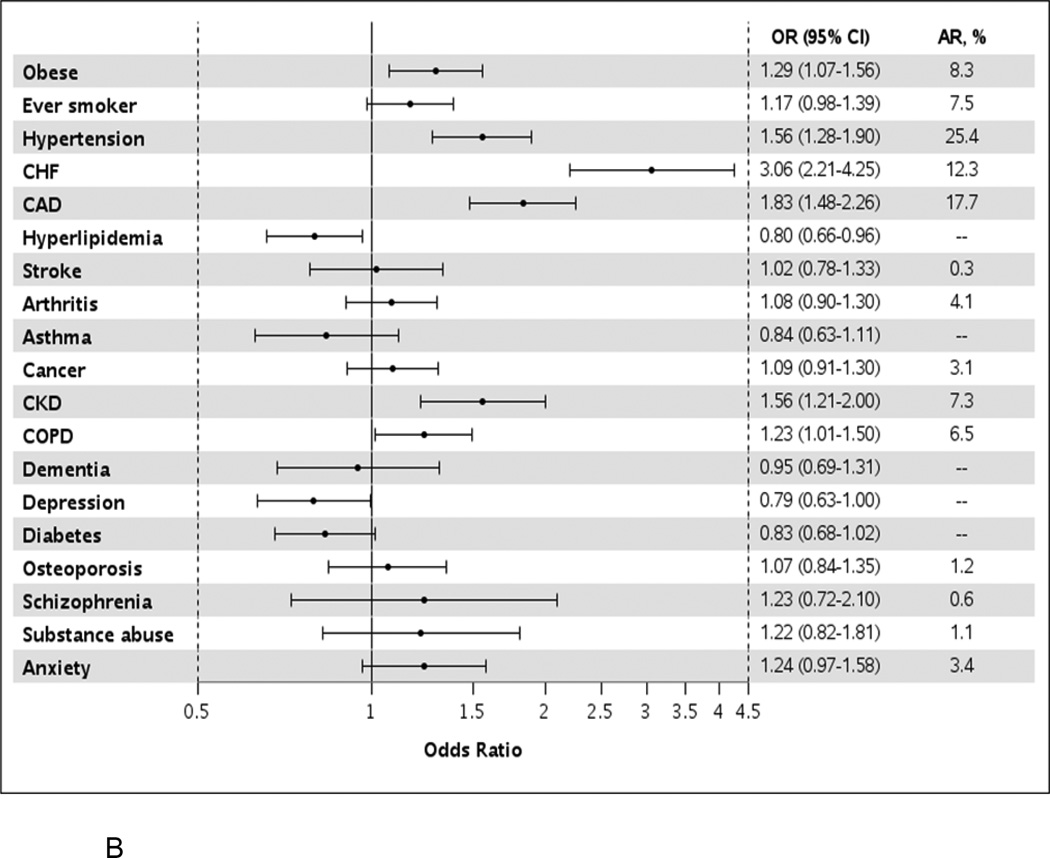
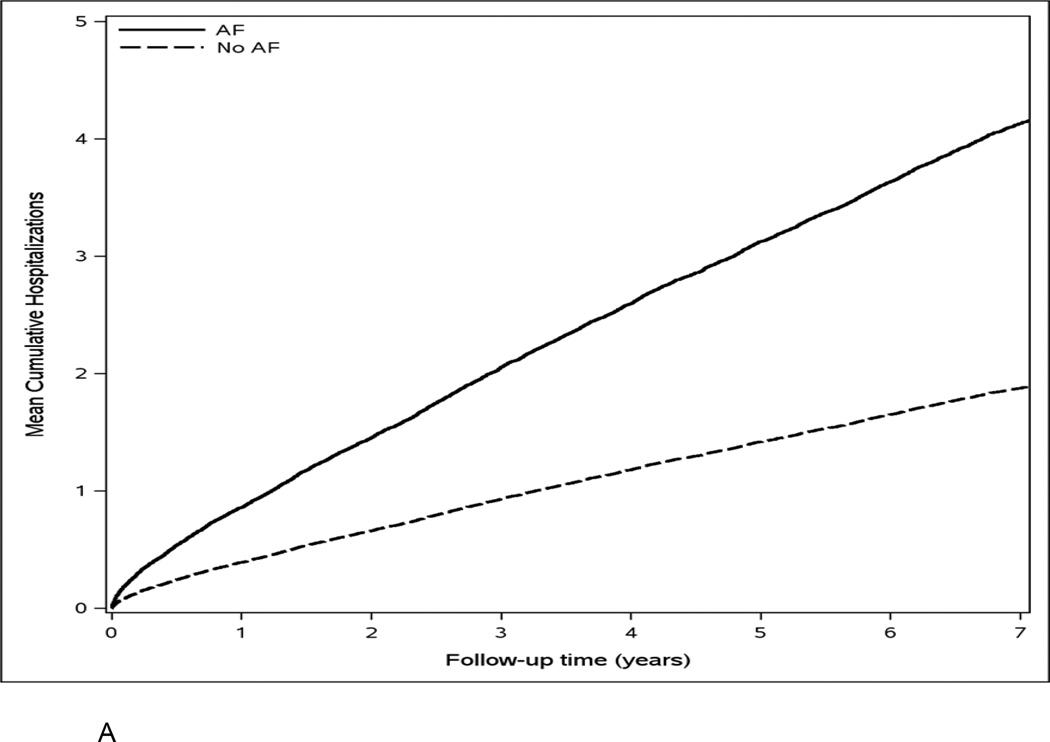
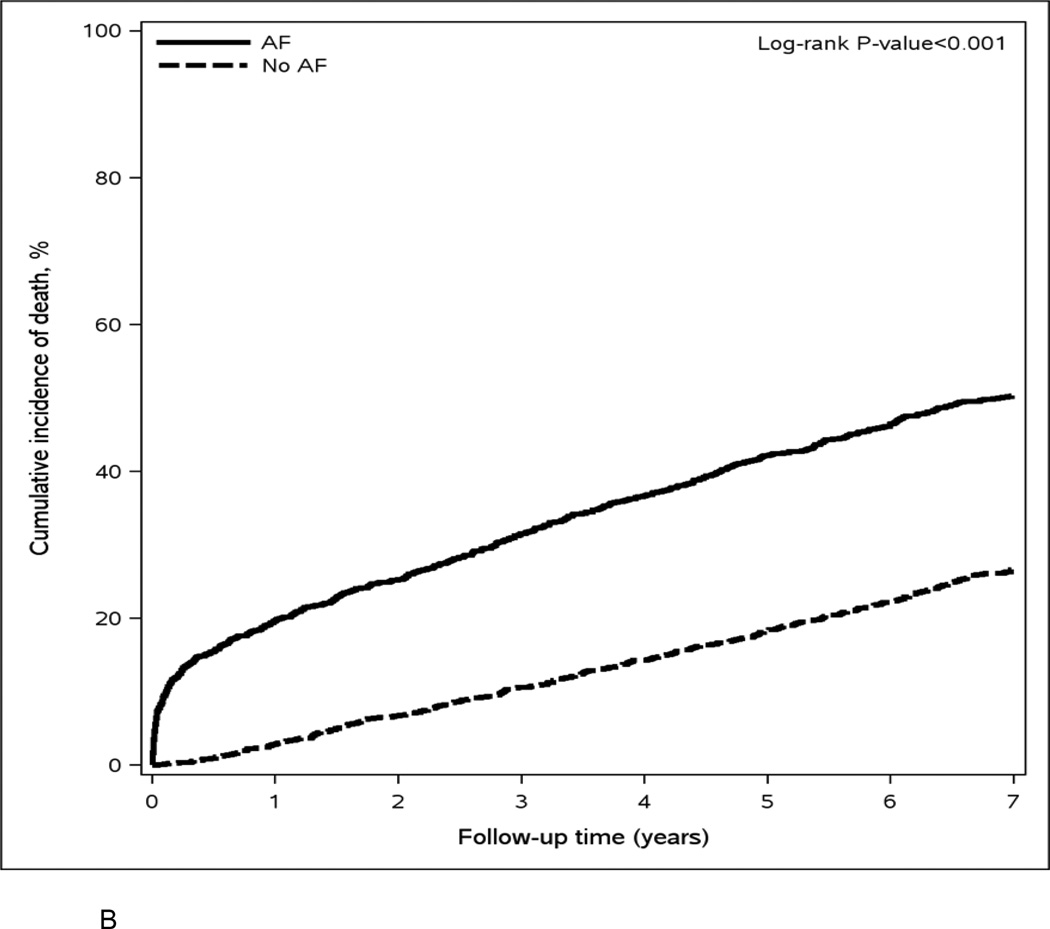
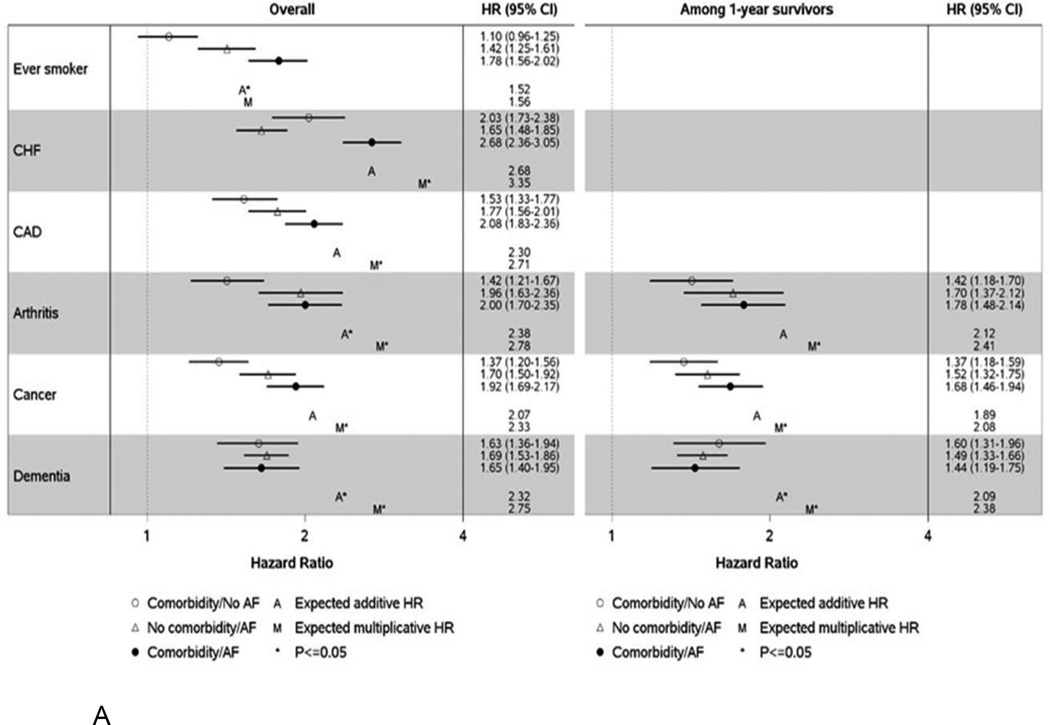
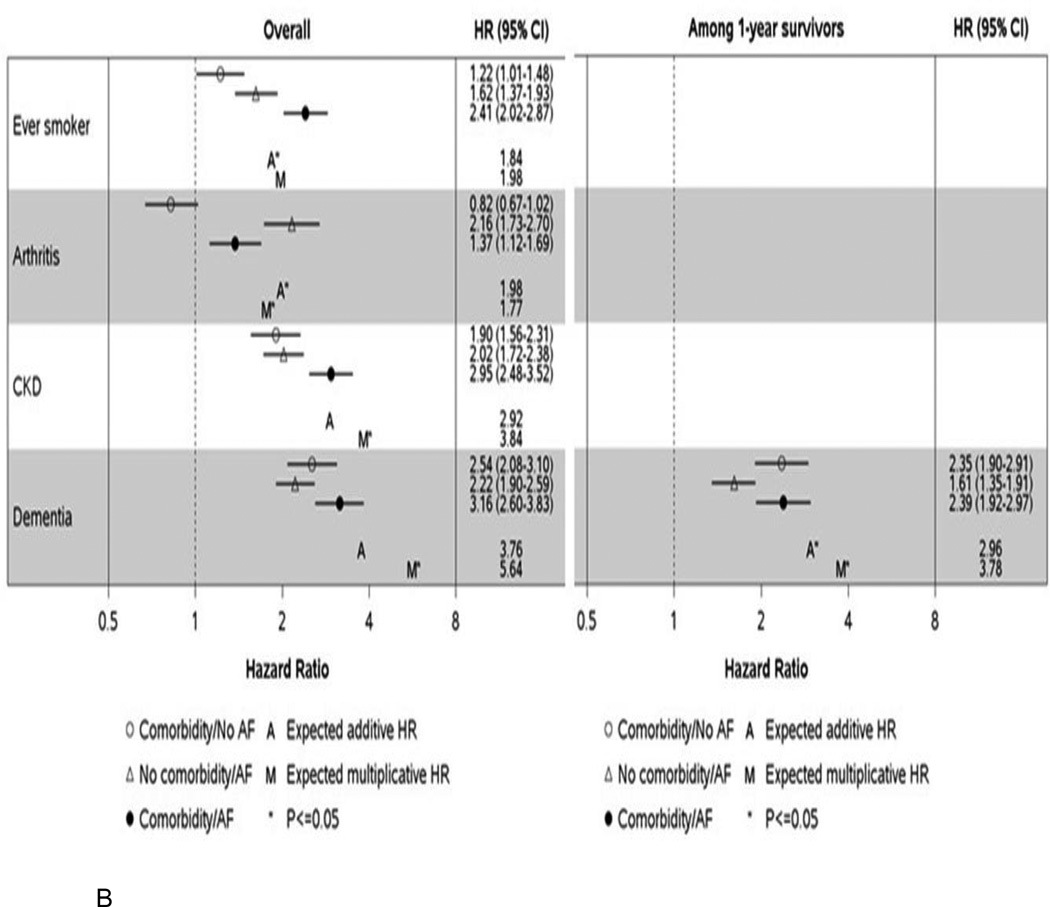
Results: AF cases had a higher prevalence of most comorbidities. Hypertension (25.4%), coronary artery disease (17.7%), and heart failure (13.3%) had the largest attributable risk of AF; these along with obesity and smoking explained 51.4% of AF. Over a mean follow-up of 6.3 years, patients with AF experienced higher rates of hospitalization and death than did population controls. However, the impact of comorbidities on hospitalization and death was generally not greater in patients with AF compared with controls, with the exception of smoking. Ever smokers with AF experienced higher-than-expected risks of hospitalization and death, with observed vs expected (assuming additivity of effects) hazard ratios compared with never smokers without AF of 1.78 (1.56-2.02) vs 1.52 for hospitalization and 2.41 (2.02-2.87) vs 1.84 for death.
Conclusions: Patients with AF have a higher prevalence of most comorbidities; however, the impact of comorbidities on hospitalization and death is generally similar in AF and controls. Smoking is a notable exception; ever smokers with AF experienced higher-than-expected risks of hospitalization and death. Thus, interventions targeting modifiable behaviors may benefit patients with AF by reducing their risk of adverse outcomes.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285(18):2370–2375. - PubMed
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114(2):119–125. - PubMed
-
- Colilla S, Crow A, Petkun W, Singer DE, Simon T, Liu X. Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am J Cardiol. 2013;112(8):1142–1147. - PubMed
-
- Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol. 2009;104(11):1534–1539. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
