

Predictors of In-hospital Postoperative Opioid Overdose After Major Elective Operations: A Nationally Representative Cohort Study
- PMID: 28267693
- PMCID: PMC6153445
- DOI: 10.1097/SLA.0000000000001945
Predictors of In-hospital Postoperative Opioid Overdose After Major Elective Operations: A Nationally Representative Cohort Study
Erratum in
-
Predictors of In-hospital Postoperative Opioid Overdose After Major Elective Operations: A Nationally Representative Cohort Study: Erratum.Ann Surg. 2017 Dec;266(6):e122. doi: 10.1097/SLA.0000000000002500. Ann Surg. 2017. PMID: 29140854 No abstract available.
Abstract
Objective: The aim of this study was to describe national trends and outcomes of in-hospital postoperative opioid overdose (OD) and identify predictors of postoperative OD.
Summary of background data: In 2000, the Joint Commission recommended making pain the 5th vital sign, increasing the focus on postoperative pain control. However, the benefits of pain management must be weighed against the potentially lethal risk of opioid OD.
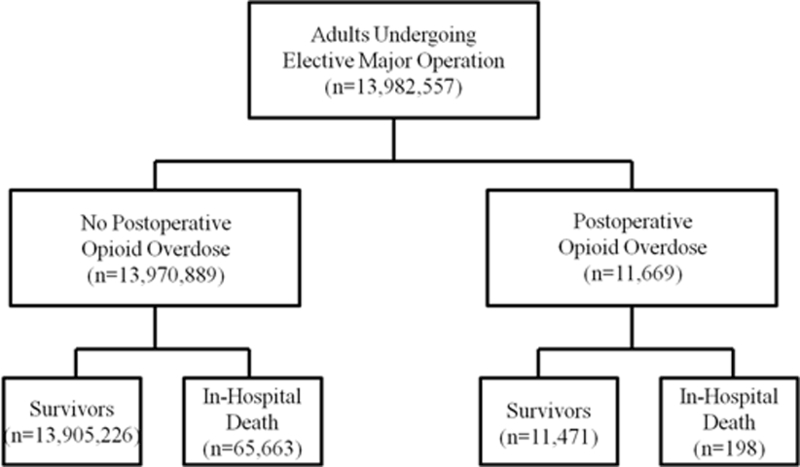
Methods: This is a retrospective multi-institutional cohort study of patients undergoing 1 of 6 major elective inpatient operation from 2002 to 2011 using the Nationwide Inpatient Sample, an approximately 20% representative sample of all United States hospital admissions. Patients with postoperative OD were identified using ICD-9 codes for poisoning from opioids or adverse effects from opioids. Multivariate logistic regression was used to identify independent predictors.
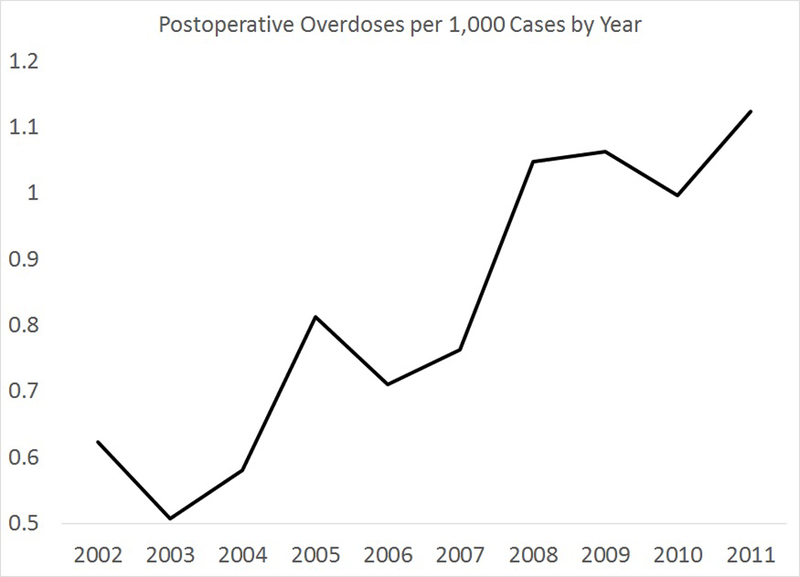
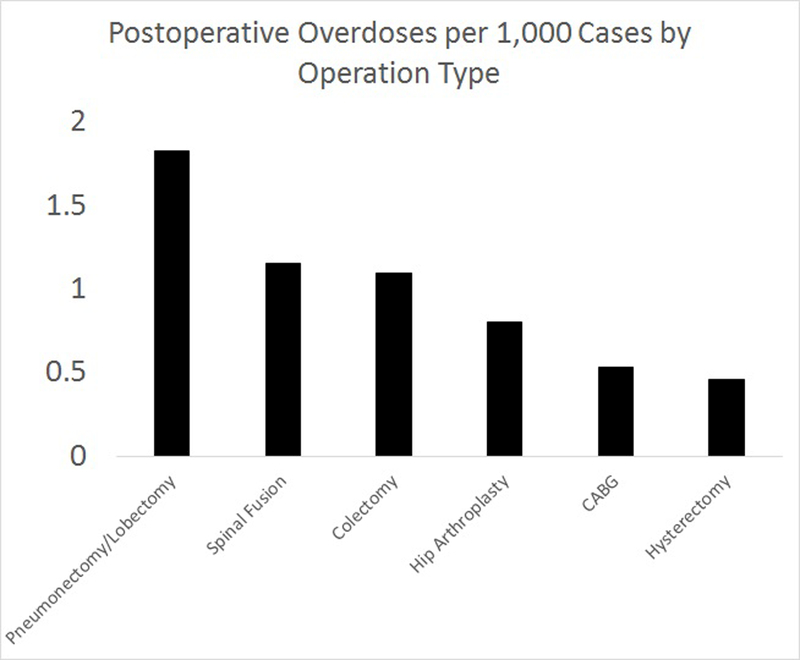
Results: Among 11,317,958 patients, 9458 (0.1%) had a postoperative OD; this frequency doubled over the study period from 0.6 to 1.1 overdoses per 1000 cases. Patients with postoperative OD died more frequently during their hospitalization (1.7% vs 0.4%, P < 0.001). Substance abuse history was the strongest predictor of OD (odds ratio = 14.8; 95% confidence interval: 12.7-17.2). Gender, age, income, geographic location, operation type, and certain comorbid diseases also predicted OD (P < 0.05). Hospital variables, including teaching status, size, and urban/rural location, did not predict postoperative OD.
Conclusions: Postoperative OD is a rare, but potentially lethal complication, with increasing incidence. Postoperative monitoring and treatment safety interventions should be thoughtfully employed to target high-risk patients and avoid this potentially fatal complication.
Figures
References
-
- Phillips DM. JCAHO pain management standards are unveiled. Joint Commission on Accreditation of Healthcare Organizations. Jama 2000;284(4):428–9. - PubMed
-
- Wells N PC, McCaffery M. Improving the Quality of Care Through Pain Assessment and Management. In: RG H, editor. Patient safety and quality: An evidence-based handbook for nurses Rockville, MD: AHRQ Publication; 2008. p. 474–502.
-
- CDC grand rounds: prescription drug overdoses -a U.S. epidemic. MMWR Morb Mortal Wkly Rep 2012;61(1):10–3. - PubMed
-
- Safe use of opioids in hospitals http://www.jointcommission.org/assets/1/18/sea_49_opioids_8_2_12_final.pdf: The Joint Commission, 2012. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
