

Defining the incidence and risk factors of colistin-induced acute kidney injury by KDIGO criteria
- PMID: 28267779
- PMCID: PMC5340380
- DOI: 10.1371/journal.pone.0173286
Defining the incidence and risk factors of colistin-induced acute kidney injury by KDIGO criteria
Abstract
Background: Acute kidney injury (AKI) remains a treatment-limiting toxicity of colistin. Recently developed clinical practice guidelines from the Kidney Disease: Improving Global Outcomes (KDIGO) group have harmonized definitions of AKI, but have not been widely applied to patients receiving colistin.
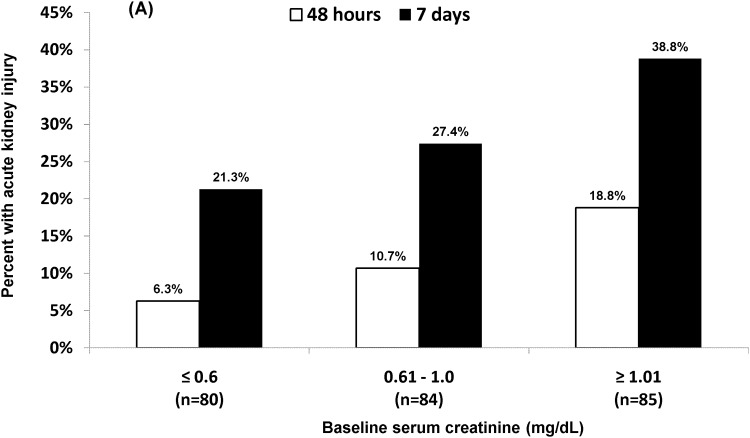
Methods: We retrospectively defined AKI by KDIGO definitions among adult patients receiving intravenous colistin for ≥ 3 days. Risk factors for AKI within 48 hours and 7 days of initiating colistin were determined by multivariable logistic regression.
Results: Among 249 patients treated with colistin, rates of AKI were 12% and 29% at 48 hours and 7 days, respectively. At 48 hours, patients in the intensive care unit were at increased risk for AKI. Within 7 days, colistin daily doses >5mg/kg, chronic liver disease, and concomitant vancomycin were independent predictors. Seven percent of patients required renal replacement therapy at a median of 5 days (range: 3-7) following colistin initiation.
Conclusion: Safe use of colistin is promoted by early detection of AKI with KDIGO criteria, avoiding nephrotoxins, and limiting duration of therapy.
Conflict of interest statement
Figures
References
-
- Garonzik SM, Li J, Thamlikitkul V, Paterson DL, Shoham S, Jacob J, et al. Population pharmacokinetics of colistin methanesulfonate and formed colistin in critically ill patients from a multicenter study provide dosing suggestions for various categories of patients. Antimicrobial agents and chemotherapy. 2011;55(7):3284–94. Epub 2011/05/11. 10.1128/AAC.01733-10 - DOI - PMC - PubMed
-
- Nation RL, Garonzik SM, Li J, Thamlikitkul V, Giamarellos-Bourboulis EJ, Paterson DL, et al. Updated US and European Dose Recommendations for Intravenous Colistin: How Do They Perform? Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2015. - PMC - PubMed
-
- Dalfino L, Puntillo F, Ondok MJ, Mosca A, Monno R, Coppolecchia S, et al. Colistin-associated Acute Kidney Injury in Severely Ill Patients: A Step Toward a Better Renal Care? A Prospective Cohort Study. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2015;61(12):1771–7. - PubMed
-
- Omrani AS, Alfahad WA, Shoukri MM, Baadani AM, Aldalbahi S, Almitwazi AA, et al. High dose intravenous colistin methanesulfonate therapy is associated with high rates of nephrotoxicity; a prospective cohort study from Saudi Arabia. Annals of clinical microbiology and antimicrobials. 2015;14:3 10.1186/s12941-015-0062-8 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
