

Multimorbidity and healthcare utilization among home care clients with dementia in Ontario, Canada: A retrospective analysis of a population-based cohort
- PMID: 28267802
- PMCID: PMC5340355
- DOI: 10.1371/journal.pmed.1002249
Multimorbidity and healthcare utilization among home care clients with dementia in Ontario, Canada: A retrospective analysis of a population-based cohort
Abstract
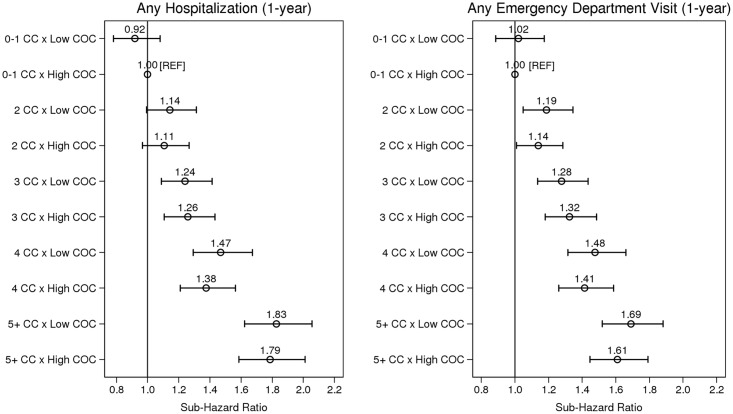
Background: For community-dwelling older persons with dementia, the presence of multimorbidity can create complex clinical challenges for both individuals and their physicians, and can contribute to poor outcomes. We quantified the associations between level of multimorbidity (chronic disease burden) and risk of hospitalization and risk of emergency department (ED) visit in a home care cohort with dementia and explored the role of continuity of physician care (COC) in modifying these relationships.
Methods and findings: A retrospective cohort study using linked administrative and clinical data from Ontario, Canada, was conducted among 30,112 long-stay home care clients (mean age 83.0 ± 7.7 y) with dementia in 2012. Multivariable Fine-Gray regression models were used to determine associations between level of multimorbidity and 1-y risk of hospitalization and 1-y risk of ED visit, accounting for multiple competing risks (death and long-term care placement). Interaction terms were used to assess potential effect modification by COC. Multimorbidity was highly prevalent, with 35% (n = 10,568) of the cohort having five or more chronic conditions. In multivariable analyses, risk of hospitalization and risk of ED visit increased monotonically with level of multimorbidity: sub-hazards were 88% greater (sub-hazard ratio [sHR] = 1.88, 95% CI: 1.72-2.05, p < 0.001) and 63% greater (sHR = 1.63; 95% CI: 1.51-1.77, p < 0.001), respectively, among those with five or more conditions, relative to those with dementia alone or with dementia and one other condition. Low (versus high) COC was associated with an increased risk of both hospitalization and ED visit in age- and sex-adjusted analyses only (sHR = 1.11, 95% CI: 1.07-1.16, p < 0.001, for hospitalization; sHR = 1.07, 95% CI: 1.03-1.11, p = 0.001, for ED visit) but did not modify associations between multimorbidity and outcomes (Wald test for interaction, p = 0.566 for hospitalization and p = 0.637 for ED visit). The main limitations of this study include use of fixed (versus time-varying) covariates and focus on all-cause rather than cause-specific hospitalizations and ED visits, which could potentially inform interventions.
Conclusions: Older adults with dementia and multimorbidity pose a particular challenge for health systems. Findings from this study highlight the need to reshape models of care for this complex population, and to further investigate health system and other factors that may modify patients' risk of health outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Alzheimer’s Association. 2015 Alzheimer’s disease facts and figures. Alzheimers Dement. 2015;11(3):332–84. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
