

Aortic shear stress in patients with bicuspid aortic valve with stenosis and insufficiency
- PMID: 28268004
- PMCID: PMC5438758
- DOI: 10.1016/j.jtcvs.2016.12.059
Aortic shear stress in patients with bicuspid aortic valve with stenosis and insufficiency
Abstract
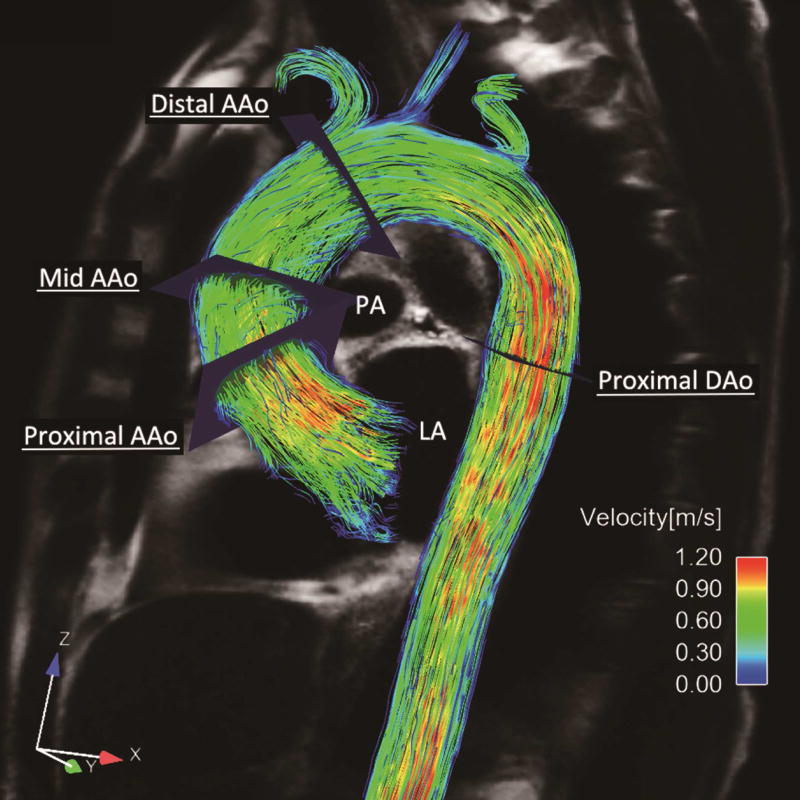
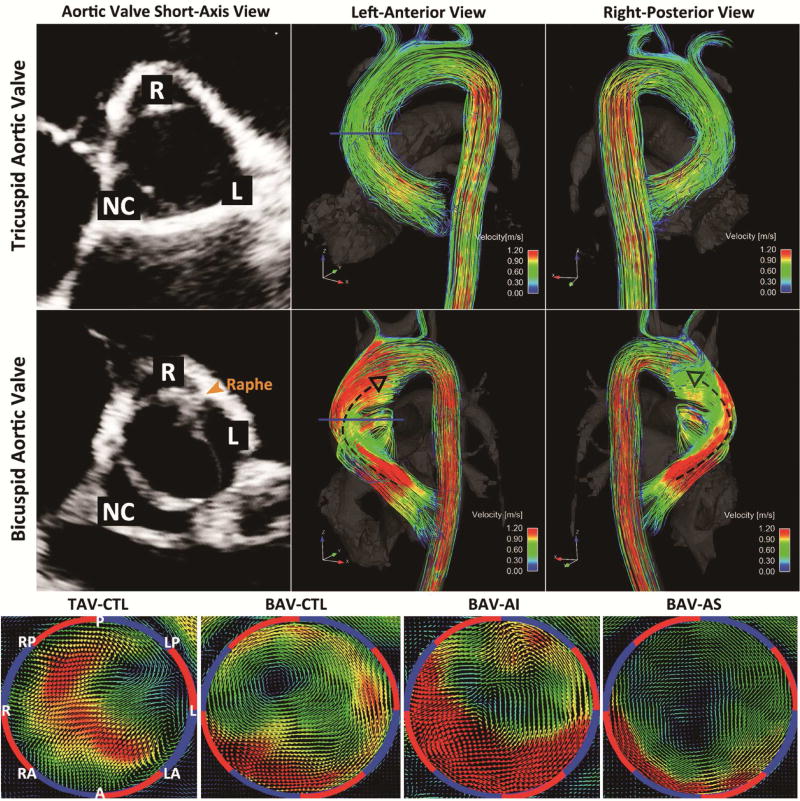
Objectives: Bicuspid aortic valve, characterized by valve malformation and risk for aortopathy, displays profound alteration in systolic aortic outflow and wall shear stress distribution. The present study performed 4-dimensional flow magnetic resonance imaging in patients with bicuspid aortic valve with right-left cusp fusion, focusing on the impact of valve function on hemodynamic status within the ascending aorta.
Methods: Four-dimensional flow magnetic resonance imaging was performed in 50 subjects with right-left bicuspid aortic valve and 15 age- and aortic size-matched controls with tricuspid aortic valve. Patients with bicuspid aortic valve were categorized into 3 groups according to their aortic valve function as follows: bicuspid aortic valve with no more than mild aortic valve dysfunction (bicuspid aortic valve control, n = 20), bicuspid aortic valve with severe aortic insufficiency (n = 15), and bicuspid aortic valve with severe aortic stenosis (n = 15).
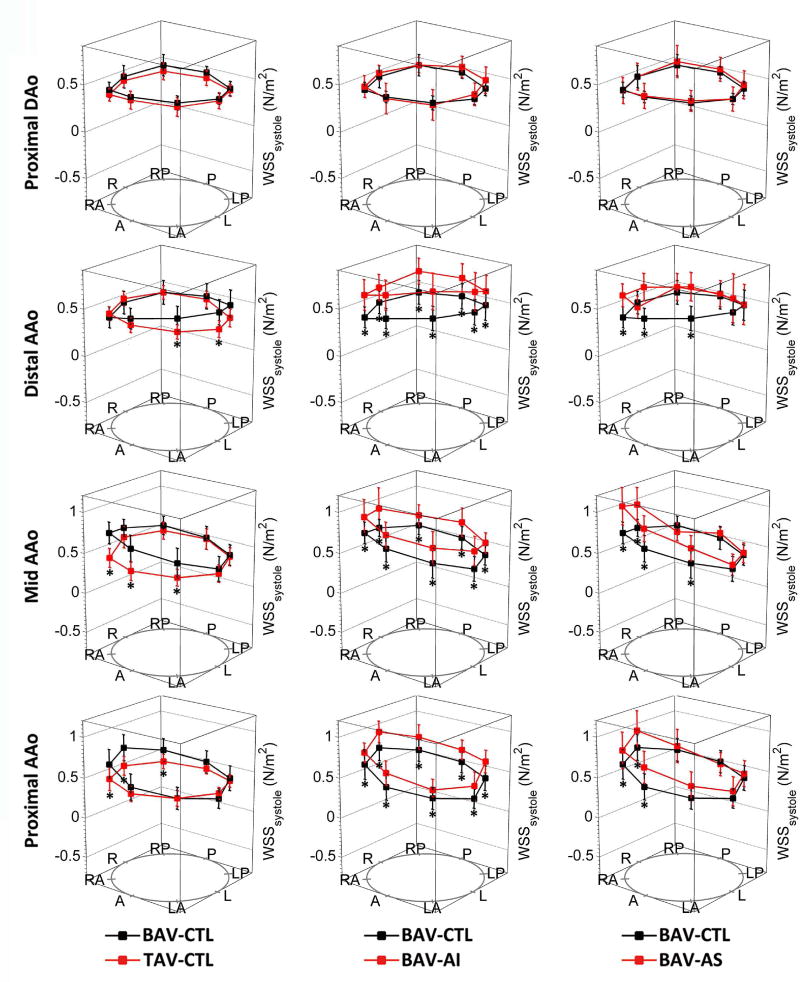
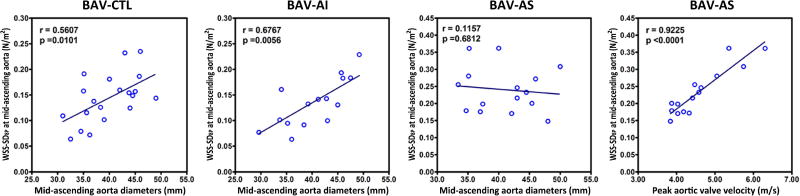
Results: All patients with right-left bicuspid aortic valve exhibited peak wall shear stress at the right-anterior position of the ascending aorta (bicuspid aortic valve vs trileaflet aortic valve at the right-anterior position: 0.91 ± 0.23 N/m2 vs 0.43 ± 0.12 N/m2, P < .001) with no distinct alteration between bicuspid aortic valve with severe aortic insufficiency and bicuspid aortic valve with severe aortic stenosis. The predominance of dilatation involving the tubular ascending aorta (82%, type 2 aortopathy) persisted, with or without valve dysfunction. Compared with bicuspid aortic valve control subjects, the bicuspid aortic valve with severe aortic insufficiency group displayed universally elevated wall shear stress (0.75 ± 0.12 N/m2 vs 0.57 ± 0.09 N/m2, P < .01) in the ascending aorta, which was associated with elevated cardiac stroke volume (P < .05). The bicuspid aortic valve with severe aortic stenosis group showed elevated flow eccentricity in the form of significantly increased standard deviation of circumferential wall shear stress, which correlated with markedly increased peak aortic valve velocity (P < .01).
Conclusions: The location of peak aortic wall shear stress and type of aortopathy remained homogeneous among patients with right-left bicuspid aortic valve irrespective of valve dysfunction. Severe aortic insufficiency or stenosis resulted in further elevated aortic wall shear stress and exaggerated flow eccentricity.
Keywords: bicuspid aortic valve; magnetic resonance imaging; wall shear stress.
Copyright © 2017 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Form follows function.J Thorac Cardiovasc Surg. 2017 Jun;153(6):1261-1262. doi: 10.1016/j.jtcvs.2017.02.046. Epub 2017 Mar 9. J Thorac Cardiovasc Surg. 2017. PMID: 28351478 No abstract available.
-
The sheer stress of deciding when to replace the aorta in bicuspid valve disease.J Thorac Cardiovasc Surg. 2017 Jun;153(6):1273-1274. doi: 10.1016/j.jtcvs.2017.03.018. Epub 2017 Mar 18. J Thorac Cardiovasc Surg. 2017. PMID: 28377120 No abstract available.
References
-
- Markl M, Chan FP, Alley MT, Wedding KL, Draney MT, Elkins CJ, et al. Time-resolved three-dimensional phase-contrast MRI. J Magn Reson Imaging. 2003;17:499–506. - PubMed
-
- Stalder AF, Russe MF, Frydrychowicz A, Bock J, Hennig J, Markl M. Quantitative 2D and 3D phase contrast MRI: optimized analysis of blood flow and vessel wall parameters. Magn Reson Med. 2008;60:1218–31. - PubMed
-
- Fedak PW, Verma S, David TE, Leask RL, Weisel RD, Butany J. Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation. 2002;106:900–4. - PubMed
-
- Tadros TM, Klein MD, Shapira OM. Ascending aortic dilatation associated with bicuspid aortic valve: pathophysiology, molecular biology, and clinical implications. Circulation. 2009;119:880–90. - PubMed
-
- Wang Y, Wu B, Dong L, Wang C, Shu X. Type A aortic dissection in patients with bicuspid or tricuspid aortic valves: a retrospective comparative study in 288 Chinese patients. Eur J Cardiothorac Surg. 2013;44:172–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
