

Application of the Third International Consensus Definitions for Sepsis (Sepsis-3) Classification: a retrospective population-based cohort study
- PMID: 28268067
- PMCID: PMC5449202
- DOI: 10.1016/S1473-3099(17)30117-2
Application of the Third International Consensus Definitions for Sepsis (Sepsis-3) Classification: a retrospective population-based cohort study
Abstract
Background: The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) present clinical criteria for the classification of patients with sepsis. We investigated incidence and long-term outcomes of patients diagnosed with these classifications, which are currently unknown.
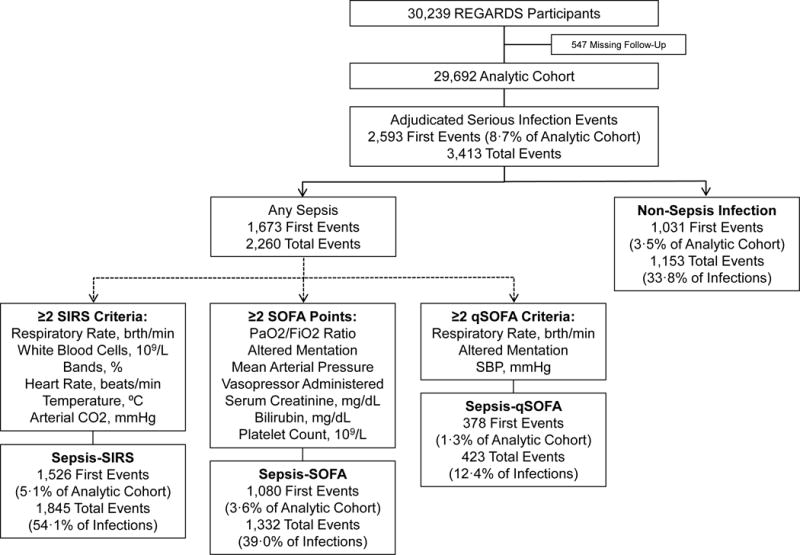
Methods: We did a retrospective analysis using data from 30 239 participants from the USA who were aged at least 45 years and enrolled in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) cohort. Patients were enrolled between Jan 25, 2003, and Oct 30, 2007, and we identified hospital admissions from Feb 5, 2003, to Dec 31, 2012, and applied three classifications: infection and systemic inflammatory response syndrome (SIRS) criteria, elevated sepsis-related organ failure assessment (SOFA) score from Sepsis-3, and elevated quick SOFA (qSOFA) score from Sepsis-3. We estimated incidence during the study period, in-hospital mortality, and 1-year mortality.
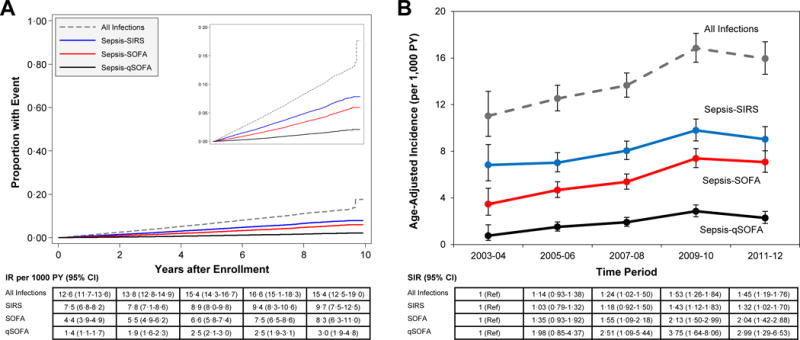
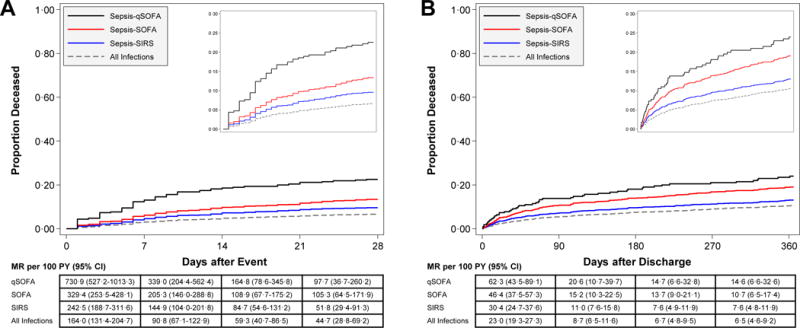
Findings: Of 2593 first infection events, 1526 met SIRS criteria, 1080 met SOFA criteria, and 378 met qSOFA criteria. Incidence was 8·2 events (95% CI 7·8-8·7) per 1000 person-years for SIRS, 5·8 events (5·4-6·1) per 1000 person-years for SOFA, and 2·0 events (1·8-2·2) per 1000 person-years for qSOFA. In-hospital mortality was higher for patients with an elevated qSOFA score (67 [23%] of 295 patients died) than for those with an elevated SOFA score (125 [13%] of 960 patients died) or who met SIRS criteria (128 [9%] of 1392 patients died). Mortality at 1 year after discharge was also highest for patients with an elevated qSOFA score (29·4 deaths [95% CI 22·3-38·7] per 100 person-years) compared with those with an elevated SOFA score (22·6 deaths [19·2-26·6] per 100 person-years) or those who met SIRS criteria (14·7 deaths [12·5-17·2] per 100 person-years).
Interpretation: SIRS, SOFA, and qSOFA classifications identified different incidences and mortality. Our findings support the use of the SOFA and qSOFA classifications to identify patients with infection who are at elevated risk of poor outcomes. These classifications could be used in future epidemiological assessments and studies of patients with infection.
Funding: National Institute for Nursing Research, National Center for Research Resources, and National Institute of Neurological Disorders and Stroke.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Dr. Safford reports investigator initiated research from Amgen. Dr. Shapiro reports research funding from Siemens, Rapid Pathogen Screening, ThermoFisher, and the National Institutes of Health, in addition to consulting for Cheetah Medical and Cyon. All others have no disclosures.
Figures

Comment in
-
Using Sepsis-3 to identify infected patients with high mortality risk.Lancet Infect Dis. 2017 Jun;17(6):573-575. doi: 10.1016/S1473-3099(17)30118-4. Epub 2017 Mar 4. Lancet Infect Dis. 2017. PMID: 28268066 No abstract available.
-
Defining sepsis: inspiring proposals meet practical realities.Lancet Infect Dis. 2017 Jun;17(6):577-578. doi: 10.1016/S1473-3099(17)30267-0. Lancet Infect Dis. 2017. PMID: 28555575 No abstract available.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Critical care medicine. 2001;29(7):1303–10. - PubMed
-
- Wang HE, Shapiro NI, Angus DC, Yealy DM. National estimates of severe sepsis in United States emergency departments. Critical care medicine. 2007;35(8):1928–36. - PubMed
-
- Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000–2012. JAMA : the journal of the American Medical Association. 2014;311(13):1308–16. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. The New England journal of medicine. 2003;348(16):1546–54. - PubMed
-
- Iwashyna TJ, Angus DC. Declining case fatality rates for severe sepsis: good data bring good news with ambiguous implications. JAMA : the journal of the American Medical Association. 2014;311(13):1295–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
