

Epidemiology and disease characteristics of systemic sclerosis-related pulmonary arterial hypertension: results from a real-life screening programme
- PMID: 28270192
- PMCID: PMC5341425
- DOI: 10.1186/s13075-017-1250-z
Epidemiology and disease characteristics of systemic sclerosis-related pulmonary arterial hypertension: results from a real-life screening programme
Abstract
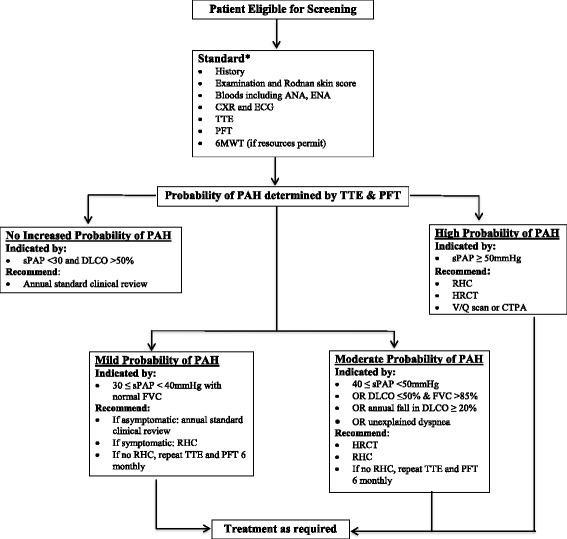
Background: Pulmonary arterial hypertension (PAH) is the leading cause of death in systemic sclerosis (SSc). Annual screening with echocardiogram (ECHO) is recommended. We present the methodological aspects of a PAH screening programme in a large Australian SSc cohort, the epidemiology of SSc-PAH in this cohort, and an evaluation of factors influencing physician adherence to PAH screening guidelines.
Methods: Patient characteristics and results of PAH screening were determined in all patients enrolled in a SSc longitudinal cohort study. Adherence to PAH screening guidelines was assessed by a survey of Australian rheumatologists. Summary statistics, chi-square tests, univariate and multivariable logistic regression were used to determine the associations of risk factors with PAH.
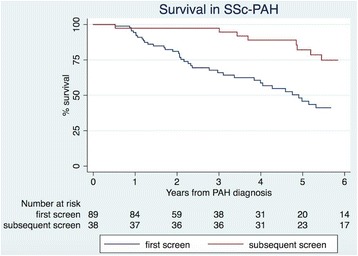
Results: Among 1636 patients with SSc, 194 (11.9%) had PAH proven by right-heart catheter. Of these, 160 were detected by screening. The annual incidence of PAH was 1.4%. Patients with PAH diagnosed on subsequent screens, compared with patients in whom PAH was diagnosed on first screen, were more likely to have diffuse SSc (p = 0.03), be in a better World Health Organisation (WHO) Functional Class at PAH diagnosis (p = 0.01) and have less advanced PAH evidenced by higher mean six-minute walk distance (p = 0.03), lower mean pulmonary arterial pressure (p = 0.009), lower mean pulmonary vascular resistance (p = 0.006) and fewer non-trivial pericardial effusions (p = 0.03). Adherence to annual PAH screening using an ECHO-based algorithm was poor among Australian rheumatologists, with less than half screening their patients with SSc of more than ten years disease duration.
Conclusion: PAH is a common complication of SSc. Physician adherence to PAH screening recommendations remains poor. Identifying modifiable barriers to screening may improve adherence and ultimately patient outcomes.
Keywords: Pulmonary arterial hypertension; Scleroderma; Screening algorithm; Systemic sclerosis.
Figures
References
-
- Marie I, Jouen F, Hellot MF, Levesque H. Anticardiolipin and anti-beta2 glycoprotein I antibodies and lupus-like anticoagulant: prevalence and significance in systemic sclerosis. Br J Dermatol. 2008;158(1):141–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
