

Cafedrine/Theodrenaline (20:1) Is an Established Alternative for the Management of Arterial Hypotension in Germany-a Review Based on a Systematic Literature Search
- PMID: 28270765
- PMCID: PMC5318387
- DOI: 10.3389/fphar.2017.00068
Cafedrine/Theodrenaline (20:1) Is an Established Alternative for the Management of Arterial Hypotension in Germany-a Review Based on a Systematic Literature Search
Abstract
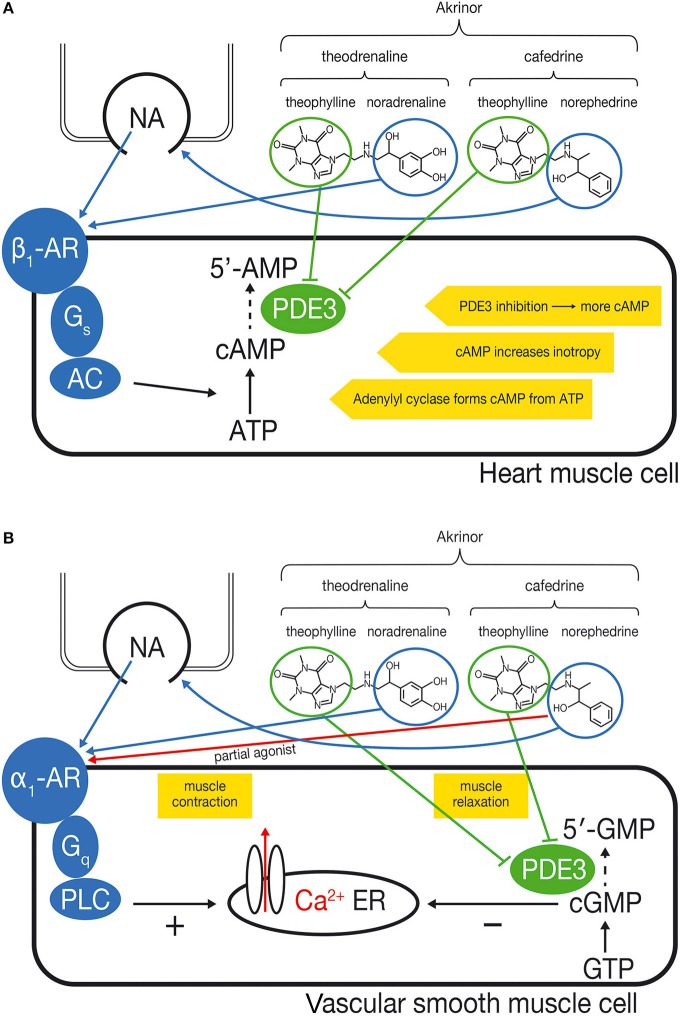
A 20:1 combination of cafedrine:theodrenaline (Akrinor®) is widely used in Germany for the treatment of hypotensive states during anesthesia and in emergency medicine. Although this drug formulation has been available since 1963, there are few studies relating to its use and many of the data are only available in German. In this article, we summarize the available data and propose mechanisms for the effects of cafedrine/theodrenaline on cardiac muscle cells and vascular smooth muscle cells. Cafedrine/theodrenaline leads to a rapid increase in mean arterial pressure that is characterized by increased cardiac preload, stroke volume, and cardiac output. Systemic vascular resistance and heart rate remain mostly unchanged. Factors which impact the effects of cafedrine/theodrenaline are gender, high arterial pressure at baseline, use of β-blockers, and heart failure. Importantly, the drug is frequently used in obstetric anesthesia without detrimental effects on umbilical cord pH or APGAR score.
Keywords: arterial hypotension: treatment; cafedrine/theodrenaline drug combination; heart frequency; inotropy; obstetric anesthesia; spinal hypotension: treatment.
Figures
References
-
- Ahlquist R. P. (1967). Development of the concept of alpha and beta adrenotropic receptors. Ann. N.Y Acad. Sci. 139, 549–552. - PubMed
-
- Bartels O., Junge O., Tropf G. (1978). Medikamentöse schock-therapie. Fortschr. Med. 96, 653–660. - PubMed
-
- Bihler K., Birtel F. J., Gundlach G. (1972). [Effect of a blood circulation analeptic amino-alkyl-theophylline (Akrinor) on kidney function and renal electrolyte balance]. Anaesthesist 21, 428–436. - PubMed
-
- Bittar G., Friedman H. S. (1991). The arrhythmogenicity of theophylline. A multivariate analysis of clinical determinants. Chest 99, 1415–1420. - PubMed
-
- Böhmert F. (1969). Klinische Erfahrungen und experimeUntersuchungen im nichthämorrhagischen Schock. Med. Welt 12, 649–652. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources