

American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on prevention of postoperative infection within an enhanced recovery pathway for elective colorectal surgery
- PMID: 28270910
- PMCID: PMC5335800
- DOI: 10.1186/s13741-017-0059-2
American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on prevention of postoperative infection within an enhanced recovery pathway for elective colorectal surgery
Abstract
Background: Colorectal surgery (CRS) patients are an at-risk population who are particularly vulnerable to postoperative infectious complications. Infectious complications range from minor infections including simple cystitis and superficial wound infections to life-threatening situations such as lobar pneumonia or anastomotic leak with fecal peritonitis. Within an enhanced recovery pathway (ERP), there are multiple approaches that can be used to reduce the risk of postoperative infections.
Methods: With input from a multidisciplinary, international group of experts and through a focused (non-systematic) review of the literature, and use of a modified Delphi method, we achieved consensus surrounding the topic of prevention of postoperative infection in the perioperative period for CRS patients.
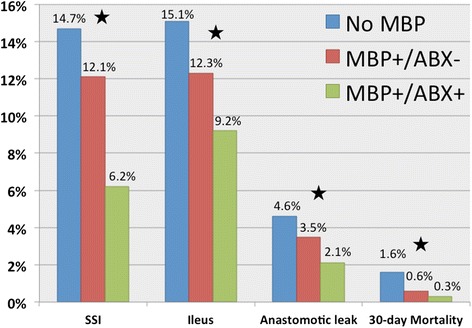
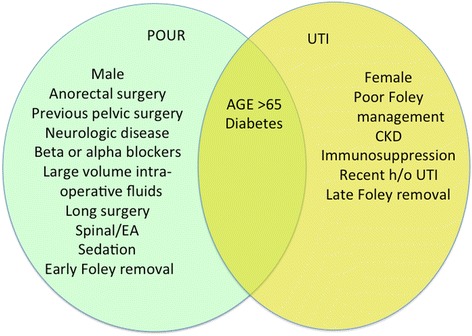
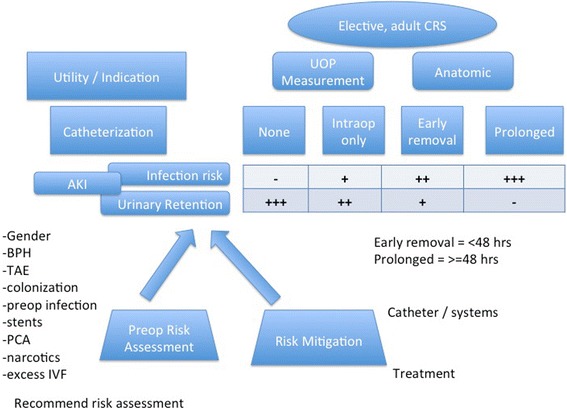
Discussion: As a part of the first Perioperative Quality Initiative (POQI-1) workgroup meeting, we sought to develop a consensus statement describing a comprehensive, yet practical, approach for reducing postoperative infections, specifically for CRS within an ERP. Surgical site infection (SSI) is the most common postoperative infection. To reduce SSI, we recommend routine use of a combined isosmotic mechanical bowel preparation with oral antibiotics before elective CRS and that infection prevention strategies (also called bundles) be routinely implemented as part of colorectal ERPs. We recommend against routine use of abdominal drains. We also give consensus guidelines for reducing pneumonia, urinary tract infection, and central line-associated bloodstream infection (CLABSI).
Keywords: Abdominal abscess; Anastomotic leak; Carepath; Catheter or line-associated bloodstream infection; Colorectal surgery; Enhanced recovery; Enhanced recovery pathway; Enhanced recovery protocol; Infection prevention; Mechanical bowel preparation; Pelvic abscess; Pneumonia; Surgical site infection; Urinary tract infection.
Figures

References
-
- Andersen HK, Lewis SJ, Thomas S. Early enteral nutrition within 24h of colorectal surgery versus later commencement of feeding for postoperative complications. Cochrane Database Syst Rev. 2006;4:CD004080. doi:10.1002/14651858.CD004080.pub2. Andersen HK, ed. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
