

Ischaemic priapism: A clinical review
- PMID: 28270944
- PMCID: PMC5330261
- DOI: 10.5152/tud.2017.59458
Ischaemic priapism: A clinical review
Abstract
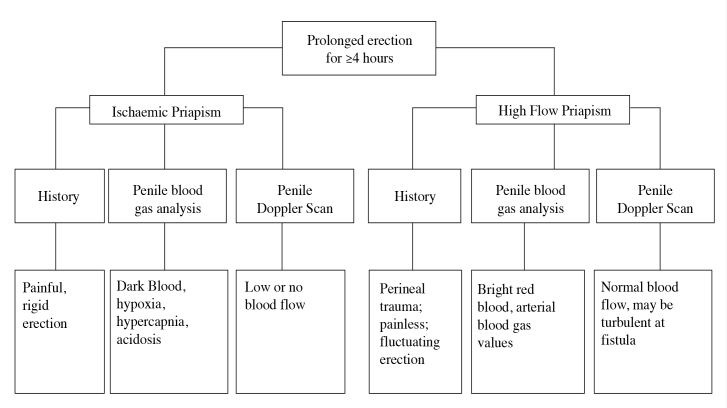
Objective: Ischaemic priapism is a rare condition characterised by little or no cavernosal blood flow, pain and rigidity of the penis. Immediate intervention is required to restore blood flow, prevent necrosis and erectile dysfunction. This review was conducted to determine the best course of treatment and identify areas in current guidelines to which improvements could be made.
Material and methods: PubMed, Ovid, MEDLINE (1946-December 2016) and the Cochrane Library were searched as sources for literature. Key studies in each of the areas of management were identified and analysed.
Results: A total of 45 articles were reviewed. The first step in treatment should be aspiration of corporeal blood. Further studies are needed to make firm recommendations as to whether irrigation should follow, as currently literature is inconclusive. If this fails to cause detumescence, sympathomimetics should be injected. The sympathomimetic of choice is phenylephrine as it is effective, specific and causes minimal cardiovascular side effects. It should be injected at a concentration of 100-500 μg/mL, with 1 mL being injected every 3-5 minutes for up to an hour (maximum 1mg in an hour). Surgical shunting is the next step, except in the cases of delayed priapism (48-72 hours duration) where immediate penile prosthesis insertion may be considered more appropriate. Distal shunts should be performed first, followed by proximal ones to minimise damage leading to erectile dysfunction. There exists little evidence recommending one shunting procedure over another. The final intervention is insertion of a penile prosthesis. Literature suggests that an inflatable prosthesis inserted immediately will yield the greatest patient satisfaction.
Conclusion: A review of the literature has highlighted areas in which further research needs to be done to make conclusive recommendations, including whether irrigation should accompany aspiration and efficacy of shunting procedures. Further studies are required to ensure that patients receive the treatment most likely to cause detumescence and maintain erectile function.
Keywords: Ischaemic; penis; priapism.
Conflict of interest statement
Conflict of Interest: No conflict of interest was declared by the authors.
Figures
References
-
- Montague D, Jarow J, Broderick D, Dmochowski R, Heaton J, Lue T, et al. American Urology Association: Guidelines on Management of Priapism. J Urol. 2003;170:1318–24. https://doi.org/10.1097/01.ju.0000087608.07371.ca. - DOI - PubMed
-
- Zacharakis E, Garaffa G, Raheem AA, Christopher AN, Muneer A, Ralph DJ. Penile prosthesis insertion in patients with refractory ischaemic priapism: early vs delayed implantation. BJU Int. 2014;114:576–81. https://doi.org/10.1111/bju.12686. - DOI - PubMed
-
- Hisasue S, Kobayashi K, Kato R, Hashimoto K, Yamashita S, Takahashi S, et al. Clinical course linkage among different priapism subtypes: Dilemma in the management strategies. Int J Urol. 2008;15:1006–10. https://doi.org/10.1111/j.1442-2042.2008.02153.x. - DOI - PubMed
-
- Berger R, Billups K, Brock G, Broderick GA, Dhabuwala CB, Goldstein I, et al. Report of the American Foundation for Urologic Disease (AFUD) Thought Leader Panel for evaluation and treatment of priapism. Int J Impotence Res. 2001;13(Suppl 5):S39–43. - PubMed
-
- Zacharakis E, Raheem AA, Freeman A, Skolarikos A, Garaffa G, Christopher AN, et al. The efficacy of the T-shunt procedure and intracavernous tunneling (snake maneuver) for refractory ischemic priapism. J Urol. 2014;191:164–8. https://doi.org/10.1016/j.juro.2013.07.034. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources