

Ultrahigh-resolution OCT imaging of the human cornea
- PMID: 28271013
- PMCID: PMC5330598
- DOI: 10.1364/BOE.8.001221
Ultrahigh-resolution OCT imaging of the human cornea
Abstract
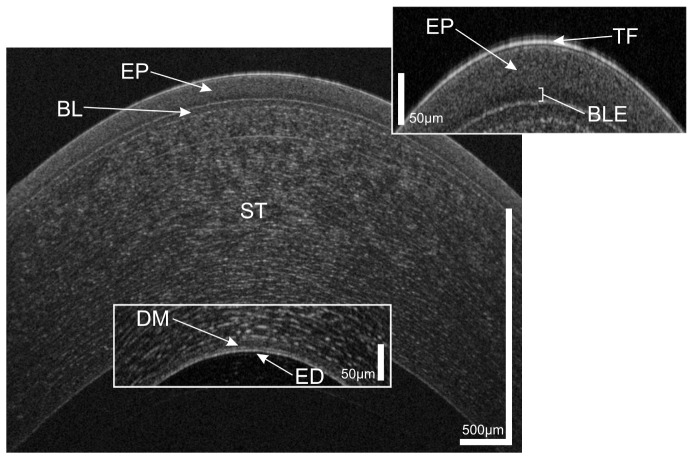
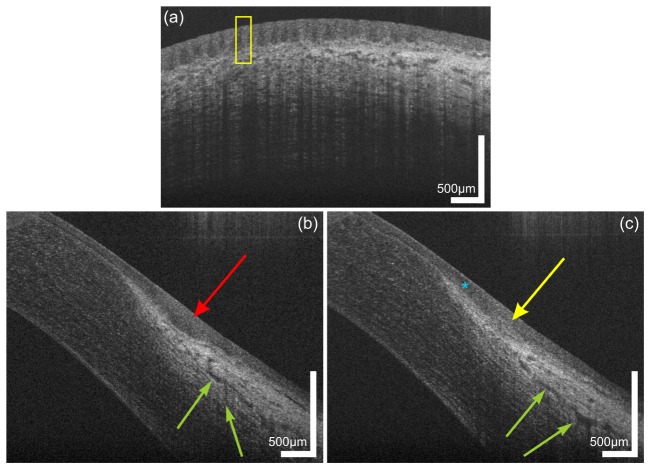
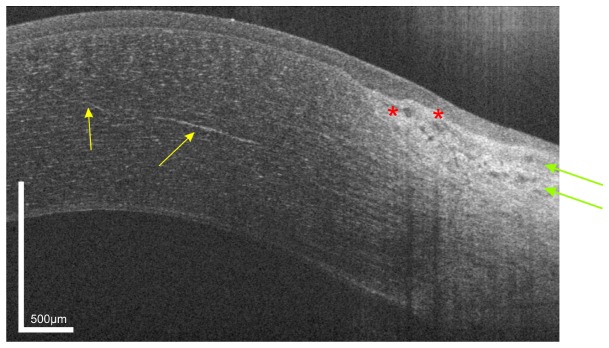
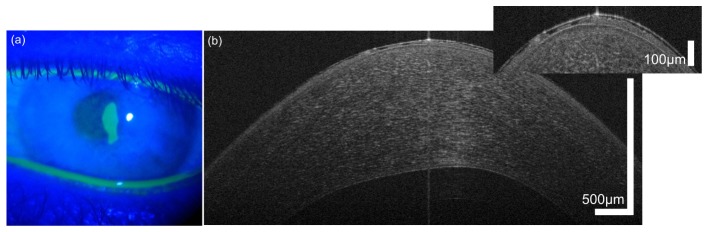
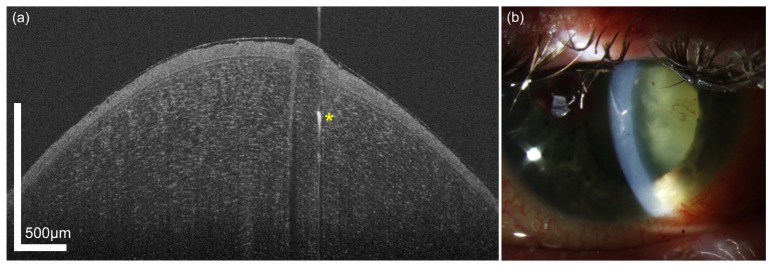
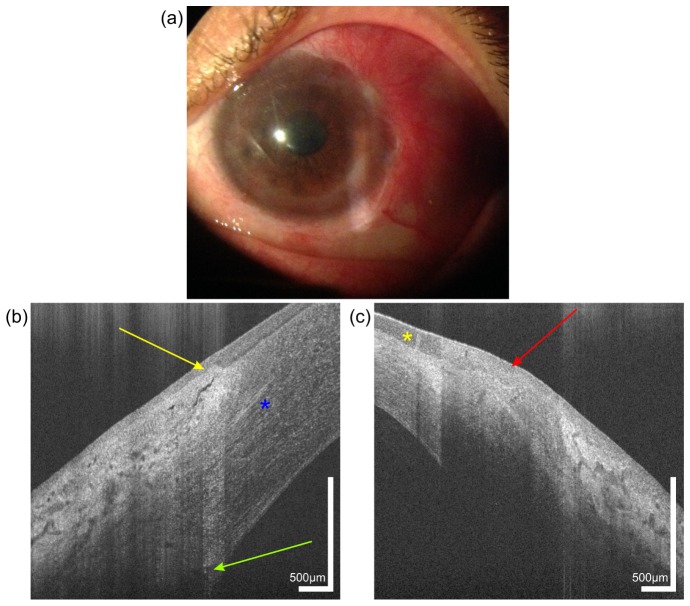
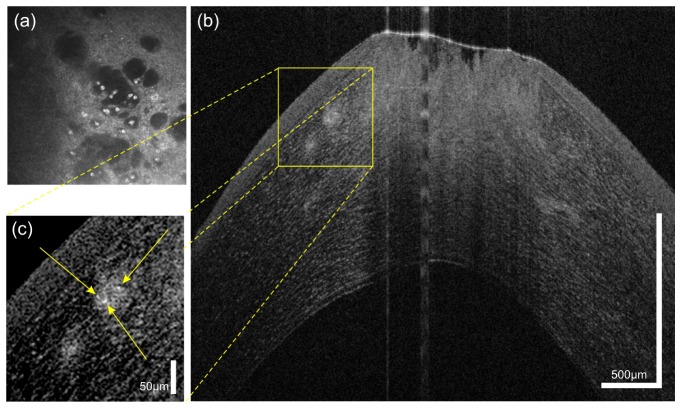
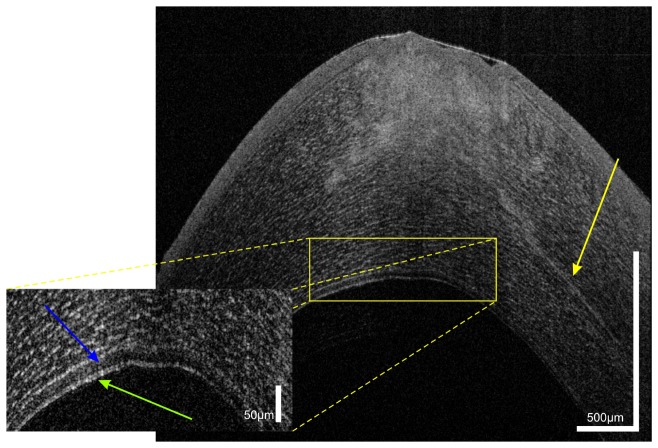
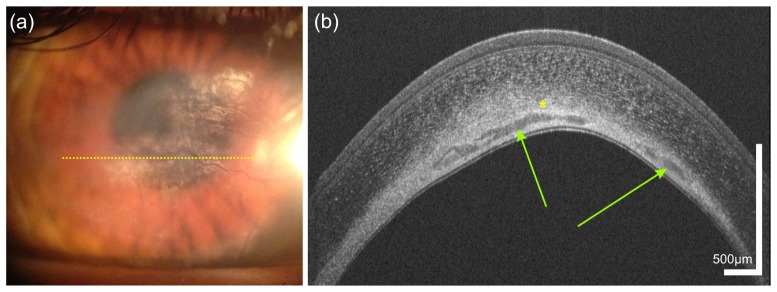
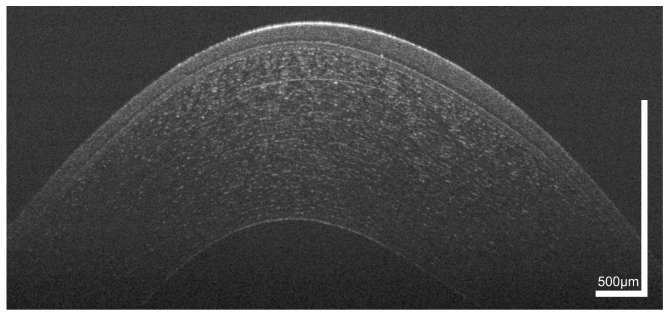
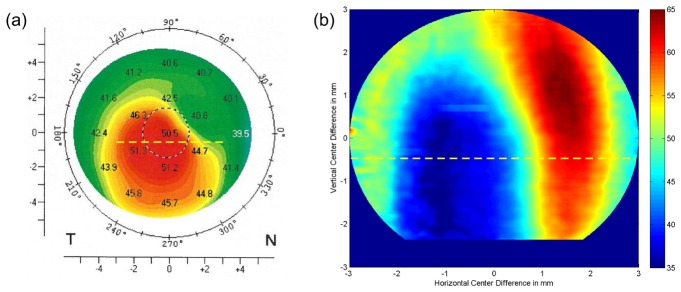
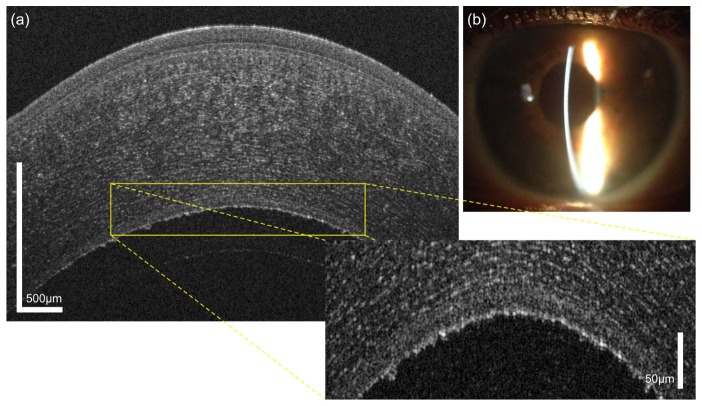
We present imaging of corneal pathologies using optical coherence tomography (OCT) with high resolution. To this end, an ultrahigh-resolution spectral domain OCT (UHR-OCT) system based on a broad bandwidth Ti:sapphire laser is employed. With a central wavelength of 800 nm, the imaging device allows to acquire OCT data at the central, paracentral and peripheral cornea as well as the limbal region with 1.2 µm x 20 µm (axial x lateral) resolution at a rate of 140 000 A-scans/s. Structures of the anterior segment of the eye, not accessible with commercial OCT systems, are visualized. These include corneal nerves, limbal palisades of Vogt as well as several corneal pathologies. Cases such as keratoconus and Fuchs's endothelial dystrophy as well as infectious changes caused by diseases like Acanthamoeba keratitis and scarring after herpetic keratitis are presented. We also demonstrate the applicability of our system to visualize epithelial erosion and intracorneal foreign body after corneal trauma as well as chemical burns. Finally, results after Descemet's membrane endothelial keratoplasty (DMEK) are imaged. These clinical cases show the potential of UHR-OCT to help in clinical decision-making and follow-up. Our results and experience indicate that UHR-OCT of the cornea is a promising technique for the use in clinical practice, but can also help to gain novel insight in the physiology and pathophysiology of the human cornea.
Keywords: (170.0110) Imaging systems; (170.4460) Ophthalmic optics and devices; (170.4500) Optical coherence tomography.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources