

Metal wear-induced pseudotumour following an endoprosthetic knee replacement for Ewing sarcoma
- PMID: 28271180
- PMCID: PMC5438826
- DOI: 10.1007/s00256-017-2610-0
Metal wear-induced pseudotumour following an endoprosthetic knee replacement for Ewing sarcoma
Abstract
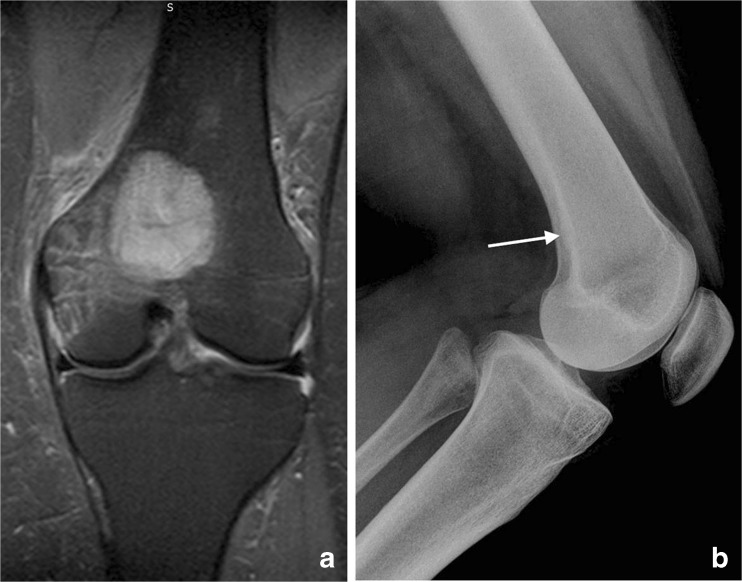
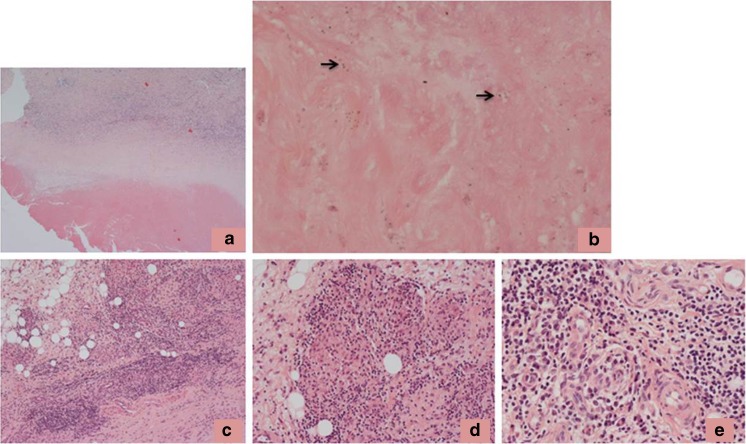
Pseudotumours are well recognised as a complication of metal-on-metal hip arthroplasties and are thought to develop on the basis of an innate and adaptive immune response to cobalt-chrome (Co-Cr) wear particles. We report a case of a large pseudotumour that developed following a knee endoprosthetic replacement (EPR) undertaken for Ewing sarcoma. The lesion contained necrotic and degenerate connective tissue in which there were numerous scattered metal wear-containing macrophages, eosinophil polymorphs, lymphocytes, plasma cells and aseptic lymphocyte-dominated vascular-associated lesion-like lymphoid aggregates. Metal ion levels were elevated. No evidence of infection or tumour was noted and it was concluded that the lesion was most likely an inflammatory pseudotumour developing on the basis of an innate and adaptive immune response to components of Co-Cr metal wear derived from the knee EPR.
Keywords: Endoprosthesis; Knee; Metal wear; Pseudotumour.
Conflict of interest statement
Funding
MV was an EU-funded visitor on the Erasmus + program
Conflicts of interest
The authors declare that they have no conflicts of interest
Figures



References
-
- Hallab NJ, Jacobs JJ. Biological effects of implant debris. Bull NYU Hosp Jt Dis. 2009;67:182–188. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
