

Examining the Dose-Response Relationship in the Veterans Health Administration's MOVE!® Weight Management Program: A Nationwide Observational Study
- PMID: 28271425
- PMCID: PMC5359164
- DOI: 10.1007/s11606-017-3992-3
Examining the Dose-Response Relationship in the Veterans Health Administration's MOVE!® Weight Management Program: A Nationwide Observational Study
Abstract
Background: For more than a decade, the Veterans Health Administration (VHA) has offered MOVE!, a comprehensive lifestyle intervention for weight management. However, there is limited knowledge to inform resource allocation decisions at the health system level-for example, the choice between reaching new veterans with weight management treatment, re-engaging veterans who have stopped attending, and/or increasing contact with current MOVE!
Objective: To inform VHA policy and planning, this VHA-wide study examines the relationship between MOVE! participation and weight outcomes.
Design: A longitudinal observational study of veterans across VHA who participated in MOVE!.
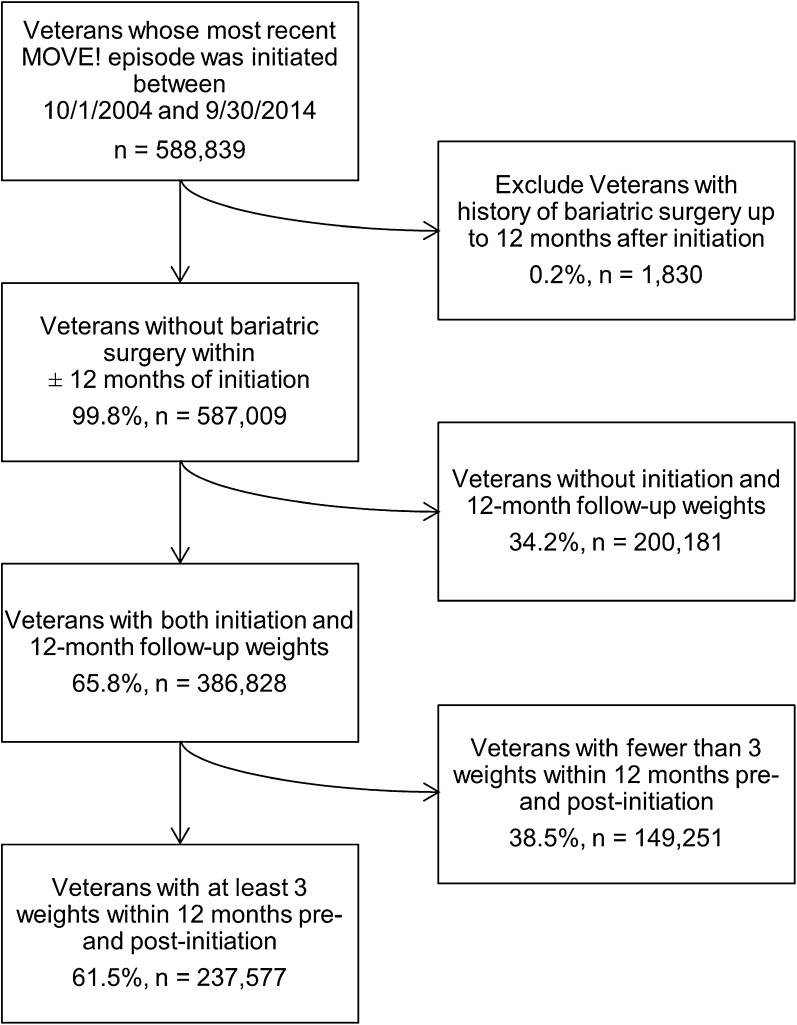
Participants: Veterans who initiated their most recent episode of MOVE! care between 2004 and 2014.
Main measures: Weight measurements were abstracted from VHA electronic health records. The primary outcome was the proportion of veterans with clinically relevant weight loss. The predictor of interest was number of MOVE! contacts during the 12 months following MOVE! initiation.
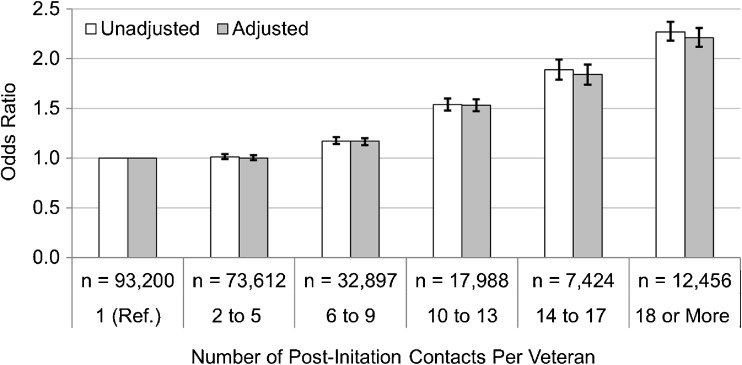
Key results: The cohort consisted of 237,577 veterans (87.4% male; mean age 54.4 years), who had 5.3 contacts on average in the 12 months following initiation. Veterans with 2-5 contacts had the same odds of achieving clinically relevant weight loss as veterans with only one contact (adjusted OR: 1.00, 95% CI: 0.98-1.03). Veterans with 6-9, 10-13, 14-17, and 18 or more contacts had significantly higher odds of clinically relevant weight loss (adjusted OR: 1.17, 95% CI: 1.13-1.20; adjusted OR: 1.53, 95% CI: 1.47-1.59; adjusted OR: 1.84, 95% CI: 1.74-1.94; adjusted OR: 2.21, 95% CI: 2.12-2.31, respectively).
Conclusions: Veterans with ≥6 MOVE! contacts in the year following treatment initiation were significantly more likely to achieve clinically relevant weight loss than those with one contact, with greater participation further increasing the odds of clinically relevant weight loss. While further characterization of weight loss predictors is needed, the VHA should provide policy guidance that supports increasing participation among veterans who have initiated MOVE!.
Keywords: behavioral science; veterans; weight management.
Conflict of interest statement
Conflict of Interest
Ms. Chan and Dr. Raffa are employees of the Department of Veterans Affairs, and have no additional conflicts of interest to declare.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans of Affairs or the United States government.
Figures
References
-
- VA/DoD 2014 Clinical Practice Guideline for the Screening and Management of Overweight and Obesity. Available at: http://www.healthquality.va.gov/guidelines/CD/obesity/CPGManagementOfOve.... Accessed 18 July 2016.
-
- LeBlanc E, O’Connor E, Whitlock EP, Patnode C, Kapka T. Screening for and Management of Obesity and Overweight in Adults. Evidence Report No. 89. AHRQ Publication No. 11-05159-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; 2011. - PubMed
-
- Moyer VA, on behalf of the U.S. Preventive Services Task Force Screening for and management of obesity in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157:373–78. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
