

MDR-TB treatment as prevention: The projected population-level impact of expanded treatment for multidrug-resistant tuberculosis
- PMID: 28273116
- PMCID: PMC5342197
- DOI: 10.1371/journal.pone.0172748
MDR-TB treatment as prevention: The projected population-level impact of expanded treatment for multidrug-resistant tuberculosis
Abstract
Background: In 2013, approximately 480,000 people developed active multidrug-resistant tuberculosis (MDR-TB), while only 97,000 started MDR-TB treatment. We sought to estimate the impact of improving access to MDR-TB diagnosis and treatment, under multiple diagnostic algorithm and treatment regimen scenarios, on ten-year projections of MDR-TB incidence and mortality.
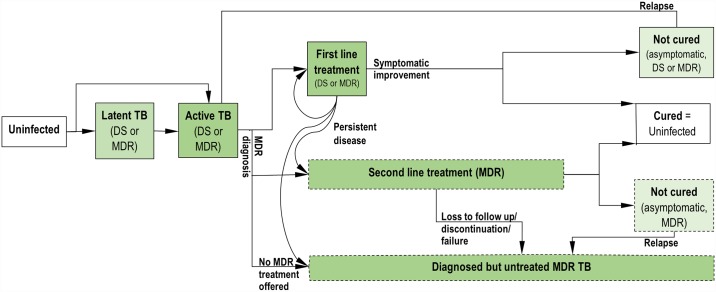
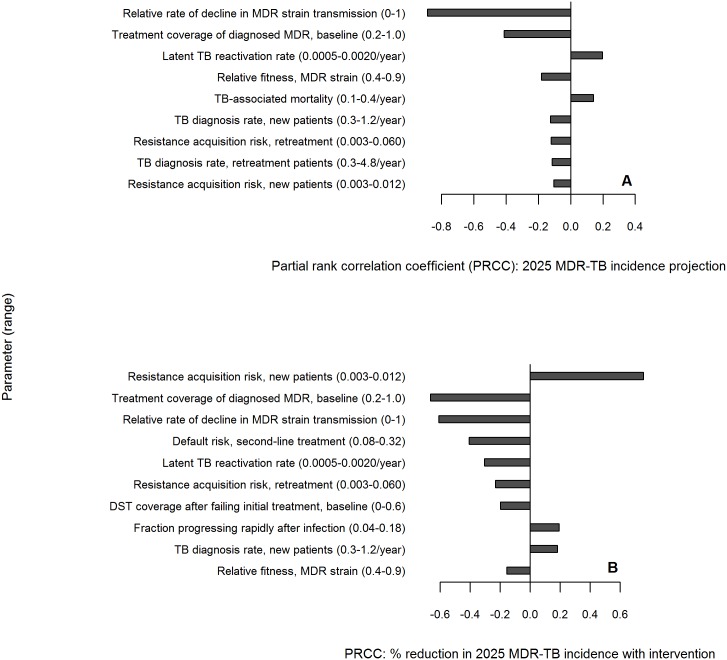
Methods: We constructed a dynamic transmission model of an MDR-TB epidemic in an illustrative East/Southeast Asian setting. Using approximate Bayesian computation, we investigated a wide array of potential epidemic trajectories consistent with current notification data and known TB epidemiology.
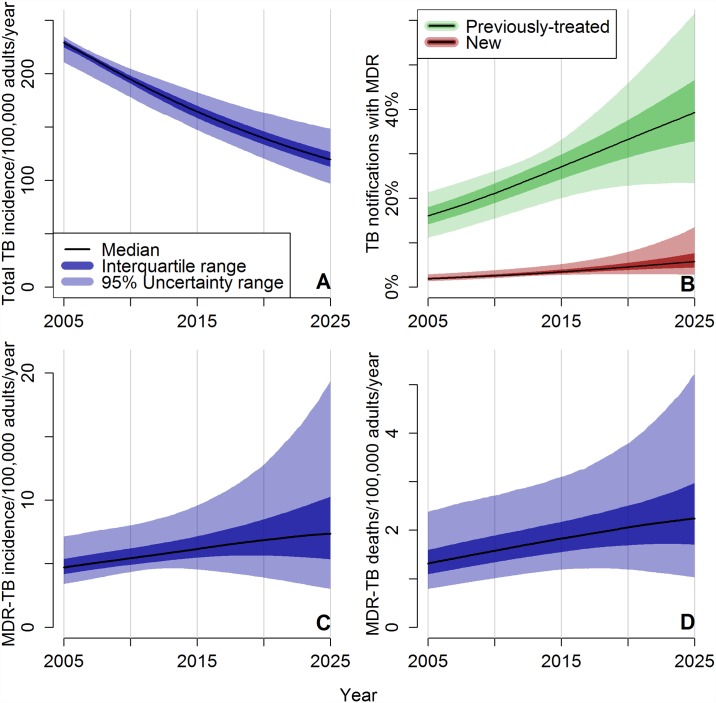
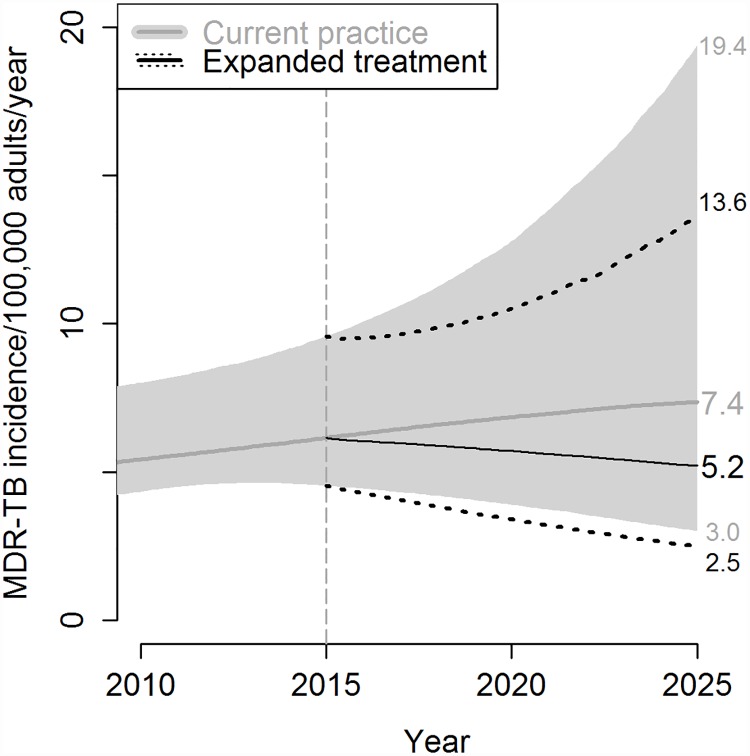
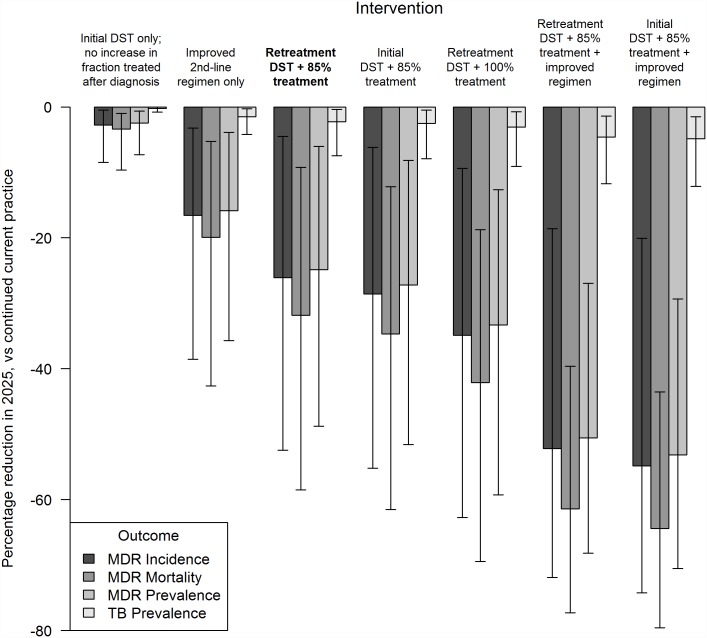
Results: Despite an overall projected decline in TB incidence, data-consistent simulations suggested that MDR-TB incidence is likely to rise between 2015 and 2025 under continued 2013 treatment practices, although with considerable uncertainty (median 17% increase, 95% Uncertainty Range [UR] -38% to +137%). But if, by 2017, all identified active TB patients with previously-treated TB could be tested for drug susceptibility, and 85% of those with MDR-TB could initiate MDR-appropriate treatment, then MDR-TB incidence in 2025 could be reduced by 26% (95% UR 4-52%) relative to projections under continued current practice. Also expanding this drug-susceptibility testing and appropriate MDR-TB treatment to treatment-naïve as well as previously-treated TB cases, by 2020, could reduce MDR-TB incidence in 2025 by 29% (95% UR 6-55%) compared to continued current practice. If this diagnosis and treatment of all MDR-TB in known active TB cases by 2020 could be implemented via a novel second-line regimen with similar effectiveness and tolerability as current first-line therapy, a 54% (95% UR 20-74%) reduction in MDR-TB incidence compared to current-practice projections could be achieved by 2025.
Conclusions: Expansion of diagnosis and treatment of MDR-TB, even using current sub-optimal second-line regimens, is expected to significantly decrease MDR-TB incidence at the population level. Focusing MDR diagnostic efforts on previously-treated cases is an efficient first-step approach.
Conflict of interest statement
Figures
References
-
- Global Tuberculosis Report 2014 [Internet]. Geneva: World Health Organization; 2014. http://www.who.int/tb/publications/global_report/en/
-
- Gosling RD, Okell L, Mosha J, Chandramohan D. The role of antimalarial treatment in the elimination of malaria. Clin Microbiol Infect Off Publ Eur Soc Clin Microbiol Infect Dis. 2011;17: 1617–1623. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
