

Parkinson's Disease: From Pathogenesis to Pharmacogenomics
- PMID: 28273839
- PMCID: PMC5372567
- DOI: 10.3390/ijms18030551
Parkinson's Disease: From Pathogenesis to Pharmacogenomics
Abstract
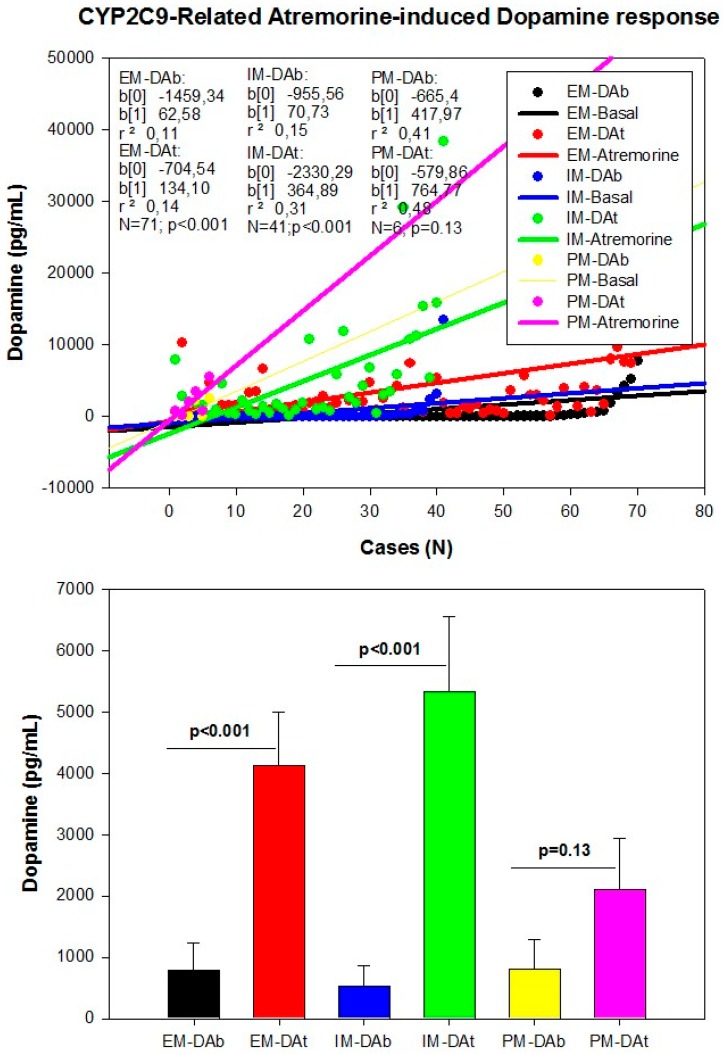
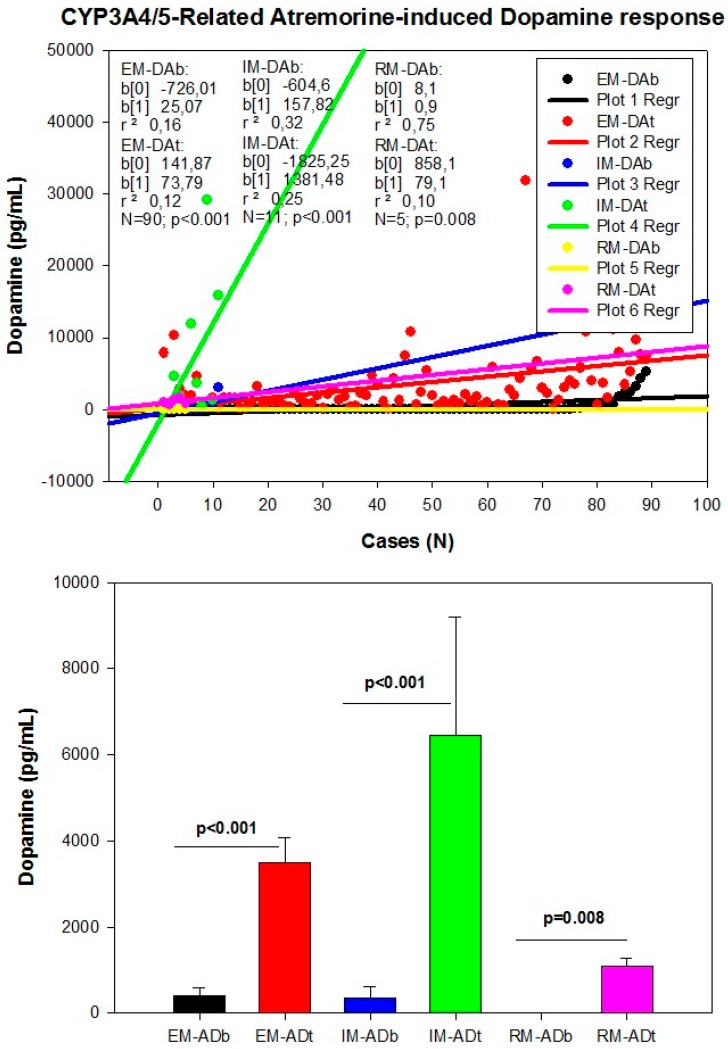
Parkinson's disease (PD) is the second most important age-related neurodegenerative disorder in developed societies, after Alzheimer's disease, with a prevalence ranging from 41 per 100,000 in the fourth decade of life to over 1900 per 100,000 in people over 80 years of age. As a movement disorder, the PD phenotype is characterized by rigidity, resting tremor, and bradykinesia. Parkinson's disease -related neurodegeneration is likely to occur several decades before the onset of the motor symptoms. Potential risk factors include environmental toxins, drugs, pesticides, brain microtrauma, focal cerebrovascular damage, and genomic defects. Parkinson's disease neuropathology is characterized by a selective loss of dopaminergic neurons in the substantia nigra pars compacta, with widespread involvement of other central nervous system (CNS) structures and peripheral tissues. Pathogenic mechanisms associated with genomic, epigenetic and environmental factors lead to conformational changes and deposits of key proteins due to abnormalities in the ubiquitin-proteasome system together with dysregulation of mitochondrial function and oxidative stress. Conventional pharmacological treatments for PD are dopamine precursors (levodopa, l-DOPA, l-3,4 dihidroxifenilalanina), and other symptomatic treatments including dopamine agonists (amantadine, apomorphine, bromocriptine, cabergoline, lisuride, pergolide, pramipexole, ropinirole, rotigotine), monoamine oxidase (MAO) inhibitors (selegiline, rasagiline), and catechol-O-methyltransferase (COMT) inhibitors (entacapone, tolcapone). The chronic administration of antiparkinsonian drugs currently induces the "wearing-off phenomenon", with additional psychomotor and autonomic complications. In order to minimize these clinical complications, novel compounds have been developed. Novel drugs and bioproducts for the treatment of PD should address dopaminergic neuroprotection to reduce premature neurodegeneration in addition to enhancing dopaminergic neurotransmission. Since biochemical changes and therapeutic outcomes are highly dependent upon the genomic profiles of PD patients, personalized treatments should rely on pharmacogenetic procedures to optimize therapeutics.
Keywords: Atremorine; Parkinson’s disease; adrenaline; antiparkinsonian drugs; dopamine; genomics; growth hormone; noradrenaline; pharmacogenetics; prolactin.
Conflict of interest statement
The author is President of EuroEspes.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
