

Six-month efficacy of platelet-rich plasma for carpal tunnel syndrome: A prospective randomized, single-blind controlled trial
- PMID: 28273894
- PMCID: PMC5427966
- DOI: 10.1038/s41598-017-00224-6
Six-month efficacy of platelet-rich plasma for carpal tunnel syndrome: A prospective randomized, single-blind controlled trial
Abstract
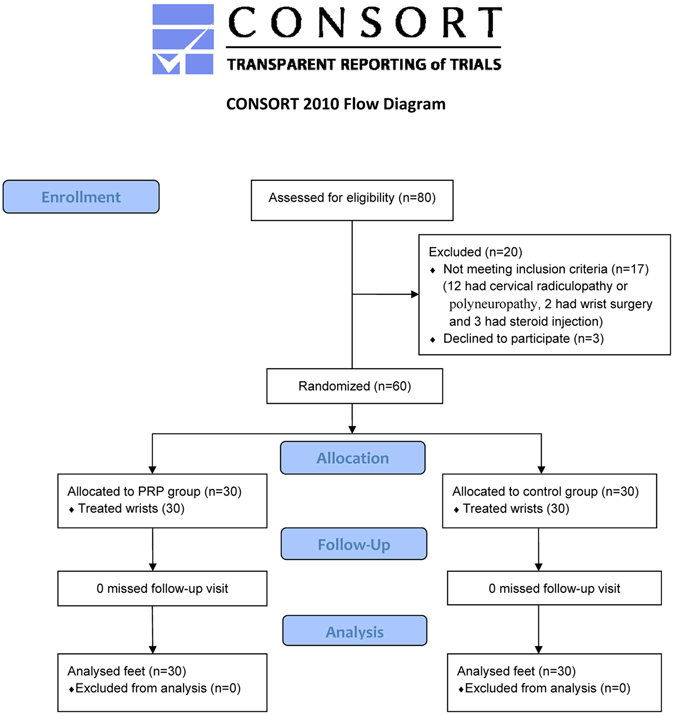
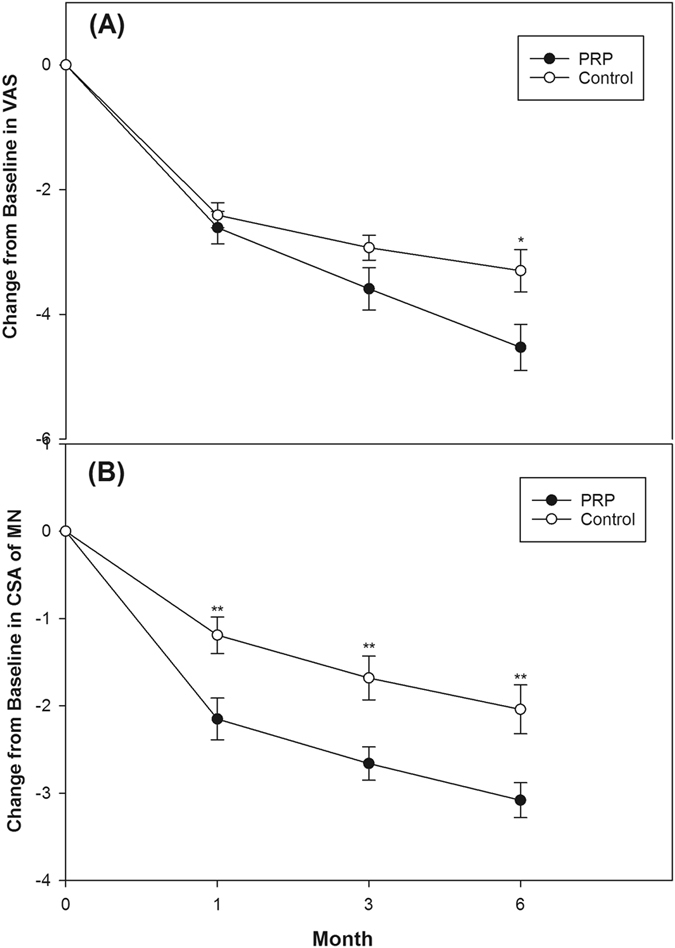
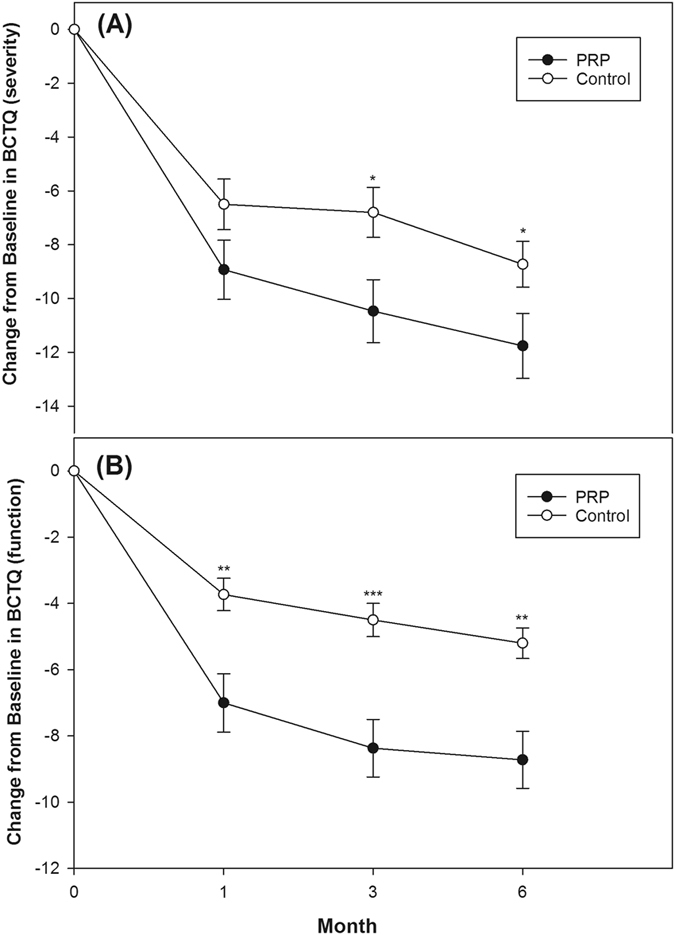
Recently, a few small reports with short follow-up period have shown clinical benefits of platelet-rich plasma (PRP) for peripheral neuropathy including one pilot study and one small, non-randomized trial in patients with carpal tunnel syndrome (CTS). Therefore, we conducted a randomized, single-blind, controlled trial to assess the 6-month effect of PRP in patients with CTS. Sixty patients with unilateral mild-to-moderate CTS were randomized into two groups of 30, namely the PRP and control groups. In the PRP group, patients were injected with one dose of 3 mL of PRP using ultrasound guidance and the control group received a night splint through the study period. The primary outcome measure was the visual analog scale (VAS) and secondary outcome measures included the Boston Carpal Tunnel Syndrome Questionnaire (BCTQ) score, the cross-sectional area (CSA) of the median nerve (MN), electrophysiological findings of the MN, and finger pinch strength. The evaluation was performed before treatment and at 1, 3, and 6 months post-injection. The PRP group exhibited a significant reduction in the VAS score, BCTQ score, and CSA of MN compared to the those of control group 6 months post-treatment (p < 0.05). Our study demonstrates that PRP is a safe modality that effectively relieves pain and improves disability in the patients with CTS.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
