

Pathophysiology and Management of Alcoholic Liver Disease: Update 2016
- PMID: 28274107
- PMCID: PMC5347641
- DOI: 10.5009/gnl16477
Pathophysiology and Management of Alcoholic Liver Disease: Update 2016
Erratum in
-
Erratum: Pathophysiology and Management of Alcoholic Liver Disease: Update 2016.Gut Liver. 2017 May 15;11(3):447. doi: 10.5009/gnl11031. Gut Liver. 2017. PMID: 28452211 Free PMC article.
Abstract
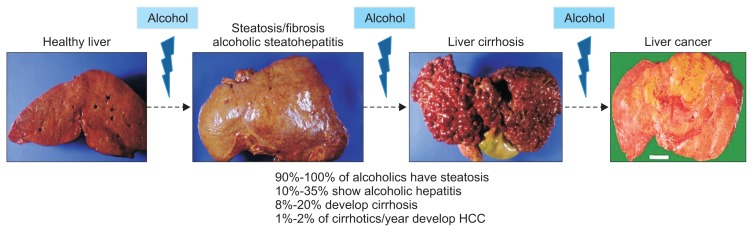
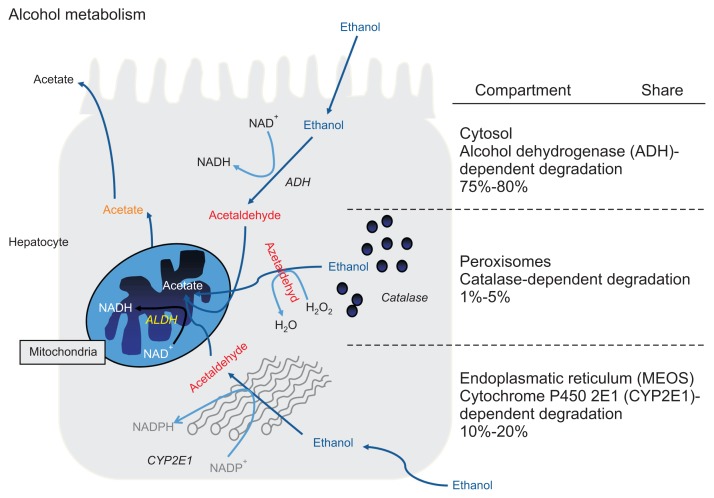
Alcoholic liver disease (ALD) is a leading cause of cirrhosis, liver cancer, and acute and chronic liver failure and as such causes significant morbidity and mortality. While alcohol consumption is slightly decreasing in several European countries, it is rising in others and remains high in many countries around the world. The pathophysiology of ALD is still incompletely understood but relates largely to the direct toxic effects of alcohol and its main intermediate, acetaldehyde. Recently, novel putative mechanisms have been identified in systematic scans covering the entire human genome and raise new hypotheses on previously unknown pathways. The latter also identify host genetic risk factors for significant liver injury, which may help design prognostic risk scores. The diagnosis of ALD is relatively easy with a panel of well-evaluated tests and only rarely requires a liver biopsy. Treatment of ALD is difficult and grounded in abstinence as the pivotal therapeutic goal; once cirrhosis is established, treatment largely resembles that of other etiologies of advanced liver damage. Liver transplantation is a sound option for carefully selected patients with cirrhosis and alcoholic hepatitis because relapse rates are low and prognosis is comparable to other etiologies. Still, many countries are restrictive in allocating donor livers for ALD patients. Overall, few therapeutic options exist for severe ALD. However, there is good evidence of benefit for only corticosteroids in severe alcoholic hepatitis, while most other efforts are of limited efficacy. Considering the immense burden of ALD worldwide, efforts of medical professionals and industry partners to develop targeted therapies in ALF has been disappointingly low.
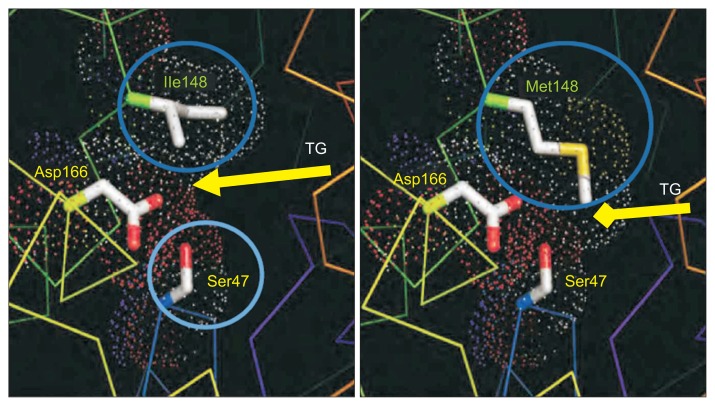
Keywords: Carcinoma, hepatocellular; Corticosteroid therapy; Hepatitis, alcoholic; Liver transplantation; Malnutrition; PNPLA3.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- World Health Organization. European status report on alcohol and health 2010. Copenhagen: WHO Regional Office for Europe; 2010.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
