

Modern Management of Anthracycline-Induced Cardiotoxicity in Lymphoma Patients: Low Occurrence of Cardiotoxicity with Comprehensive Assessment and Tailored Substitution by Nonpegylated Liposomal Doxorubicin
- PMID: 28275118
- PMCID: PMC5388379
- DOI: 10.1634/theoncologist.2016-0289
Modern Management of Anthracycline-Induced Cardiotoxicity in Lymphoma Patients: Low Occurrence of Cardiotoxicity with Comprehensive Assessment and Tailored Substitution by Nonpegylated Liposomal Doxorubicin
Abstract
Background: Anthracyclines (AC) are still undeniable drugs in lymphoma treatment, despite occasionally causing cardiotoxicity. Liposomal AC may reduce cardiotoxicity while retaining clinical efficacy; also, biomarker monitoring during chemotherapy allows early detection of cardiac damage, enabling strategies to prevent left ventricular ejection fraction (LVEF) deterioration.
Materials and methods: We conducted a prospective observational trial in a real-life population of lymphoma patients, combining advanced echocardiography and biomarkers (Troponin I [TnI]) for early detection of cardiotoxicity; we applied a prespecified policy to minimize cardiotoxicity, selecting patients with higher baseline risk to replace doxorubicin with nonpegylated liposomal doxorubicin (NPLD) and starting cardioprotective treatment when subclinical cardiotoxicity was detected.
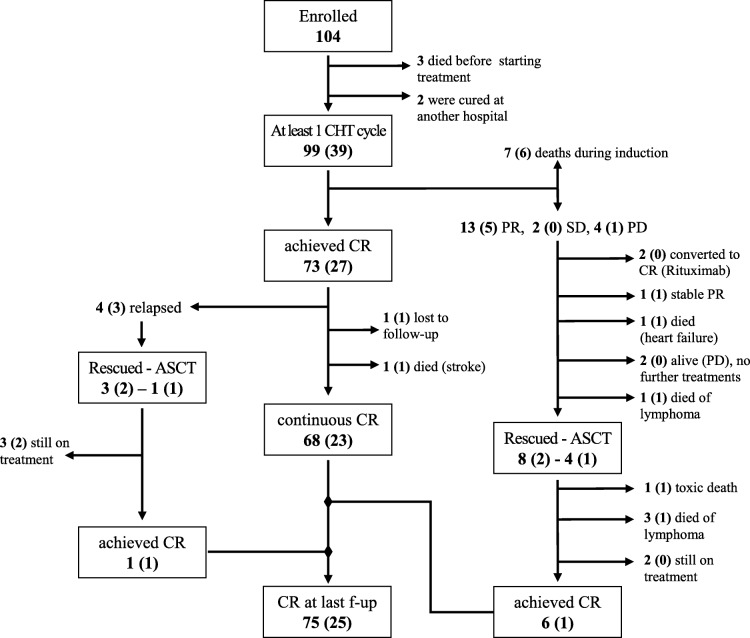
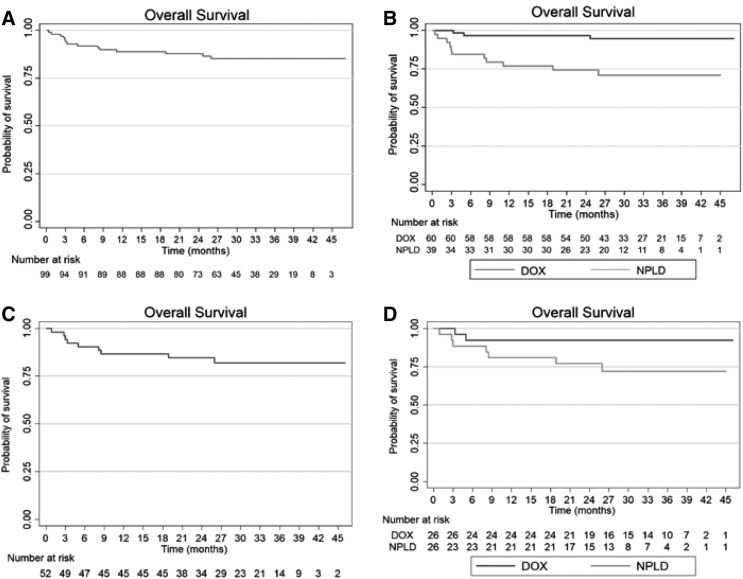
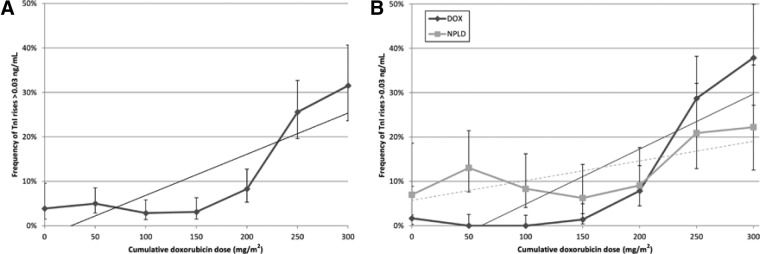
Results: Ninety-nine patients received ≥1 cycle of chemotherapy (39 with NPLD): 38 (NPLD = 34) were older than 65 years. At baseline, the NPLD subgroup had more cardiovascular risk factors and comorbidities than the doxorubicin subgroup. After treatment, echocardiographic parameters did not worsen in the NPLD subgroup; significant LVEF reduction occurred in two patients treated with doxorubicin. Over treatment course, TnI rises increased linearly in the doxorubicin subgroup but modestly in the NPLD subgroup. At doxorubicin doses >200 mg/m2 the difference was statistically significant, with more TnI rises in the doxorubicin subgroup. NPLD-treated patients did not experience higher rates of grade 3-4 adverse events. Within the diffuse large B-cell lymphomas category, we observed similar rates of complete and overall responses between doxorubicin- and NPLD-treated patients.
Conclusion: A comprehensive strategy to prevent, detect, and treat cardiotoxicity allows an optimal management of the lymphoma with low incidence of cardiac complications. The Oncologist 2017;22:422-431 IMPLICATIONS FOR PRACTICE: Despite the recent advances of targeted therapy in cancer, old cytotoxic drugs such as anthracyclines (AC) still play a fundamental role in the treatment of many lymphoma patients. We tested and validated in a real-life setting a personalized approach to prevent, detect, and treat AC-induced cardiotoxicity; biomarker monitoring was accomplished by Troponin I measurements before and after chemotherapy infusions, allowing detection of early subclinical cardiotoxicity, which was preemptively treated with cardio-protectants (beta blockers and angiotensin-converting-enzyme inhibitors). A telemedicine system allowed interdisciplinary management of the patients with an expert cardiologist. Furthermore, tailored use of liposomal AC following a prespecified policy appeared to prevent the excess cardiotoxicity expected in high-risk patients.
Keywords: Anthracyclines; Biomarkers; Cardiotoxicity; Doxorubicin; Hodgkin Disease; Lymphoma; Non‐Hodgkin.
© AlphaMed Press 2017.
Conflict of interest statement
Figures
References
-
- Di Marco A, Gaetani M, Scarpinato B. Adriamycin (NSC‐123,127): A new antibiotic with antitumor activity. Cancer Chemother Rep 1969;53:33–37. - PubMed
-
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Survivorship version 2.2015. Available at http://www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf. Accessed November 7, 2015.
-
- Von Hoff DD, Layard MW, Basa P et al. Risk factors for doxorubicin‐induced congestive heart failure. Ann Intern Med 1979;91:710–717. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
