

Clinical Trial Characteristics and Barriers to Participant Accrual: The MD Anderson Cancer Center Experience over 30 years, a Historical Foundation for Trial Improvement
- PMID: 28275168
- PMCID: PMC5354950
- DOI: 10.1158/1078-0432.CCR-16-2439
Clinical Trial Characteristics and Barriers to Participant Accrual: The MD Anderson Cancer Center Experience over 30 years, a Historical Foundation for Trial Improvement
Abstract
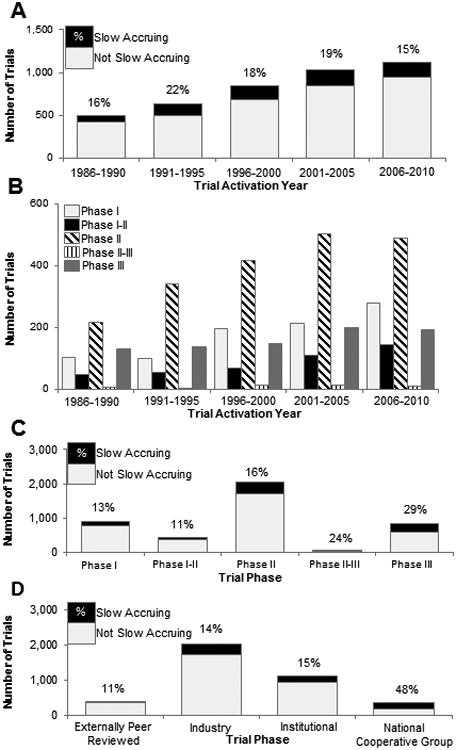
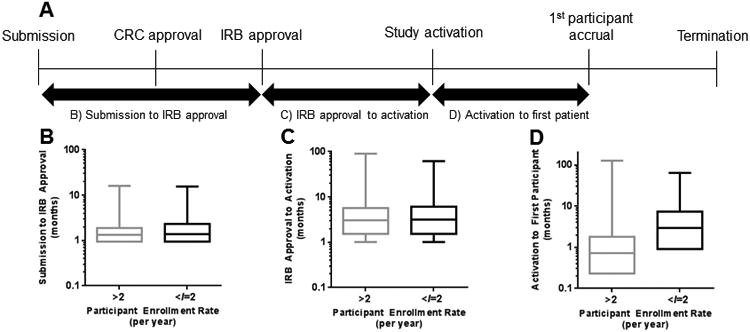
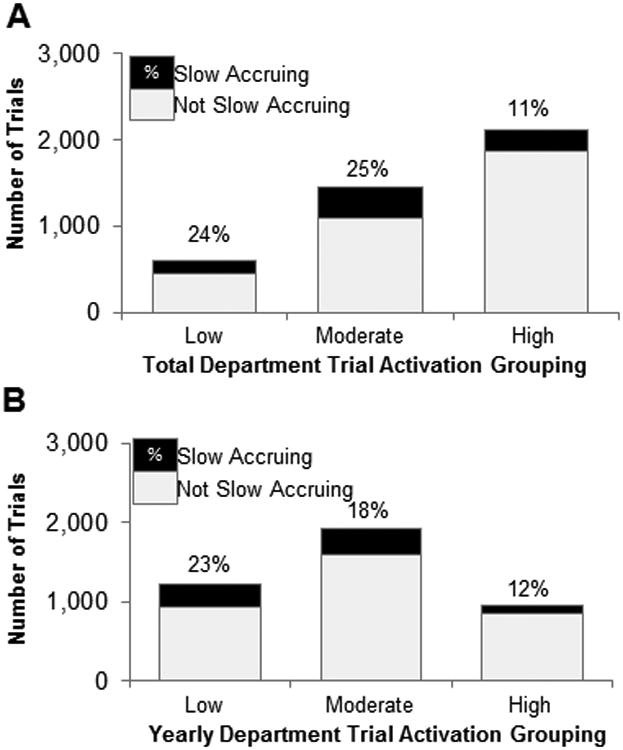
Purpose: Slow-accruing clinical trials delay the translation of basic biomedical research, contribute to increasing health care costs, and may prohibit trials from reaching their original goals.Experimental Design: We analyzed a prospectively maintained institutional database that tracks all clinical studies at the MD Anderson Cancer Center (Houston, TX). Inclusion criteria were activated phase I-III trials, maximum projected accrual ≥10 participants, and activation prior to March 25, 2011. The primary outcome was slow accrual, defined as <2 participants per year. Correlations of trial characteristics with slow accrual were assessed with logistic regression.Results: A total of 4,269 clinical trials met inclusion criteria. Trials were activated between January 5, 1981, and March 25, 2011, with a total of 145,214 participants enrolled. Median total enrolment was 16 [interquartile range (IQR), 5-34], with an average enrolment rate of 8.7 participants per year (IQR, 3.3-17.7). There were 755 (18%) trials classified as slow accruing. On multivariable analysis, slow accrual exhibited robust associations with national cooperative group trials (OR = 4.16, P < 0.0001 vs. industry sponsored), time from trial activation to first enrolment (OR = 1.13 per month, P < 0.0001), and maximum targeted accrual (OR = 0.16 per log10 increase, P < 0.0001). Recursive partitioning analysis identified trials requiring more than 70 days (2.3 months) between activation and first participant enrolment as having higher odds of slow accrual (23% vs. 5%, OR = 5.56, P < 0.0001).Conclusions: We identified factors associated with slow trial accrual. Given the lack of data on clinical trials at the institutional level, these data will help build a foundation from which targeted initiatives may be developed to improve the clinical trial enterprise. Clin Cancer Res; 23(6); 1414-21. ©2017 AACR.
©2017 American Association for Cancer Research.
Conflict of interest statement
No conflicts of interest.
Figures
References
-
- Sung NS, Crowley WF, Jr, Genel M, Salber P, Sandy L, Sherwood LM, et al. Central challenges facing the national clinical research enterprise. JAMA. 2003;289(10):1278–87. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
