

Success of photodynamic therapy in palliating patients with nonresectable cholangiocarcinoma: A systematic review and meta-analysis
- PMID: 28275308
- PMCID: PMC5323453
- DOI: 10.3748/wjg.v23.i7.1278
Success of photodynamic therapy in palliating patients with nonresectable cholangiocarcinoma: A systematic review and meta-analysis
Abstract
Aim: To perform a systematic review and meta-analysis on clinical outcomes of photodynamic therapy (PDT) in non-resectable cholangiocarcinoma.
Methods: Included studies compared outcomes with photodynamic therapy and biliary stenting (PDT group) vs biliary stenting only (BS group) in palliation of non-resectable cholangiocarcinoma. Articles were searched in MEDLINE, PubMed, and EMBASE. Pooled proportions were calculated using fixed and random effects model. Heterogeneity among studies was assessed using the I2 statistic.
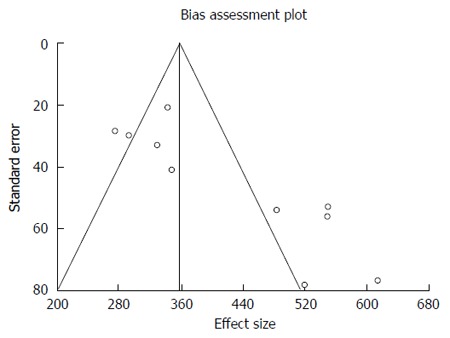
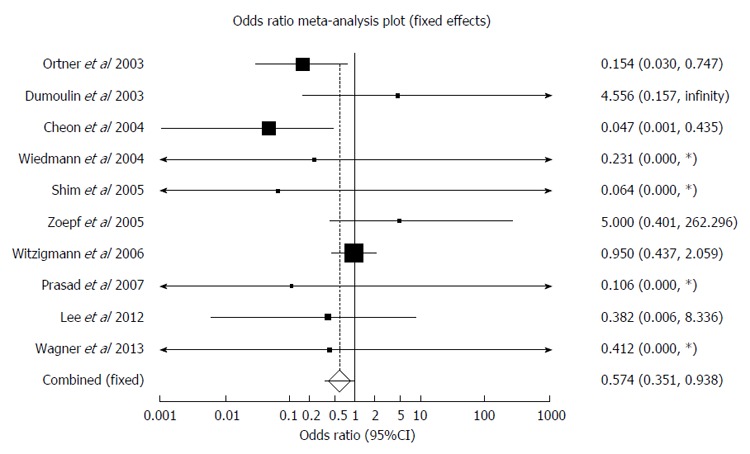
Results: Ten studies (n = 402) that met inclusion criteria were included in this analysis. The P for χ2 heterogeneity for all the pooled accuracy estimates was > 0.10. Pooled odds ratio for successful biliary drainage (decrease in bilirubin level > 50% within 7days after stenting) in PDT vs BS group was 4.39 (95%CI: 2.35-8.19). Survival period in PDT and BS groups were 413.04 d (95%CI: 349.54-476.54) and 183.41 (95%CI: 136.81-230.02) respectively. The change in Karnofsky performance scores after intervention in PDT and BS groups were +6.99 (95%CI: 4.15-9.82) and -3.93 (95%CI: -8.63-0.77) respectively. Odds ratio for post-intervention cholangitis in PDT vs BS group was 0.57 (95%CI: 0.35-0.94). In PDT group, 10.51% (95%CI: 6.94-14.72) had photosensitivity reactions that were self-limiting. Subgroup analysis of prospective studies showed similar results, except the incidence of cholangitis was comparable in both groups.
Conclusion: In palliation of unresectable cholangiocarcinoma, PDT seems to be significantly superior to BS alone. PDT should be used as an adjunct to biliary stenting in these patients.
Keywords: Biliary stenting; Meta-analysis; Outcome; Photodynamic therapy; Systematic review; Unresectable cholangiocarcinoma.
Conflict of interest statement
Conflict-of-interest statement: The authors deny any conflict of interest.
Figures







References
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis. 2004;24:115–125. - PubMed
-
- Rea DJ, Munoz-Juarez M, Farnell MB, Donohue JH, Que FG, Crownhart B, Larson D, Nagorney DM. Major hepatic resection for hilar cholangiocarcinoma: analysis of 46 patients. Arch Surg. 2004;139:514–523; discussion 523-525. - PubMed
-
- Dinant S, Gerhards MF, Rauws EA, Busch OR, Gouma DJ, van Gulik TM. Improved outcome of resection of hilar cholangiocarcinoma (Klatskin tumor) Ann Surg Oncol. 2006;13:872–880. - PubMed
-
- Hasegawa S, Ikai I, Fujii H, Hatano E, Shimahara Y. Surgical resection of hilar cholangiocarcinoma: analysis of survival and postoperative complications. World J Surg. 2007;31:1256–1263. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
