

Congenital Orbital Teratoma
- PMID: 28275597
- PMCID: PMC5318934
- DOI: 10.1159/000448144
Congenital Orbital Teratoma
Abstract
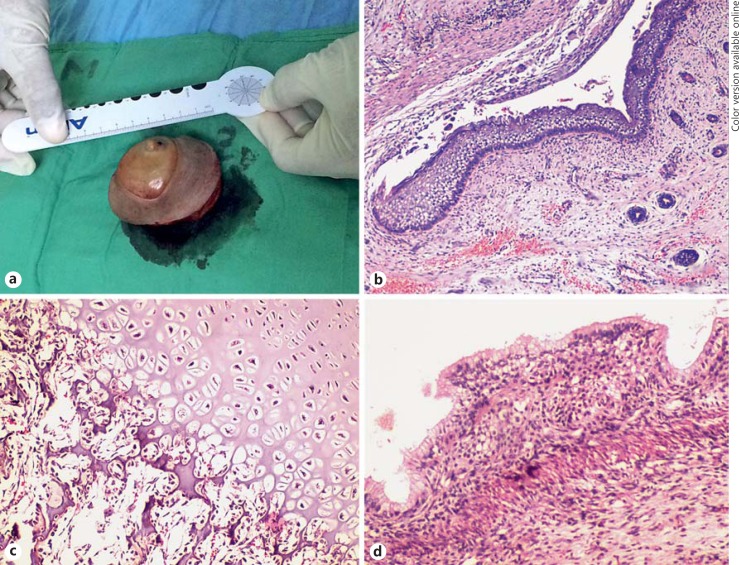
We report a case of congenital orbital teratoma. A 3-day-old male, born at 39 weeks' gestation without relevant prenatal history, presented with a large vascularized proptotic mass distorting the left midface. Laboratory studies showed elevated serum alpha-fetoprotein (12,910 ng/ml). Computed tomography showed a multiloculated heterogeneous lesion composed of hypodense and hyperdense calcified areas encompassing the whole orbital cavity with expansion of the bony walls, as well as forward displacement and compression of the eyeball without extension to surrounding structures. Clinical, imaging and laboratory features were consistent with congenital orbital teratoma. Due to pronounced proptosis with exposure keratopathy and corneal perforation, no motility of the globe and no vision in the affected eye in a resource-limited setting, the patient underwent orbital exenteration. Histopathological examination confirmed the diagnosis of mature cystic teratoma. We describe the clinical course, radiographic and histopathological findings of this rare orbital tumor.
Keywords: Congenital teratoma; Orbital tumor; Proptosis in a neonate.
Figures



References
-
- Günalp I, Gündüz K. Cystic lesions of the orbit. Int Ophthalmol. 1996;20:273–277. - PubMed
-
- Choi SH, Han YB, Lee TJ. A case of congenital orbital teratoma. Korean J Ophthalmol. 1987;1:139–144. - PubMed
-
- Grube-Pagola P, Hobart-Hernández RI, Martínez-Hernández MA, Gómez-Dorantes SM, Alderete-Vázquez G. Congenital proptosis secondary to orbital teratoma. Clinicopathological study. Arch Soc Esp Oftalmol. 2013;88:153–156. - PubMed
-
- Gnanaraj L, Skibell BC, Coret-Simon J, Halliday W, Forrest C, DeAngelis DD. Massive congenital orbital teratoma. Ophthal Plast Reconstr Surg. 2005;21:445–447. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
