

Ocular Surface Squamous Neoplasia Associated with Atopic Keratoconjunctivitis
- PMID: 28275599
- PMCID: PMC5318932
- DOI: 10.1159/000448220
Ocular Surface Squamous Neoplasia Associated with Atopic Keratoconjunctivitis
Abstract
Purpose: To describe 2 cases of invasive squamous cell carcinoma that originated in the setting of severe atopic keratoconjunctivitis (AKC).
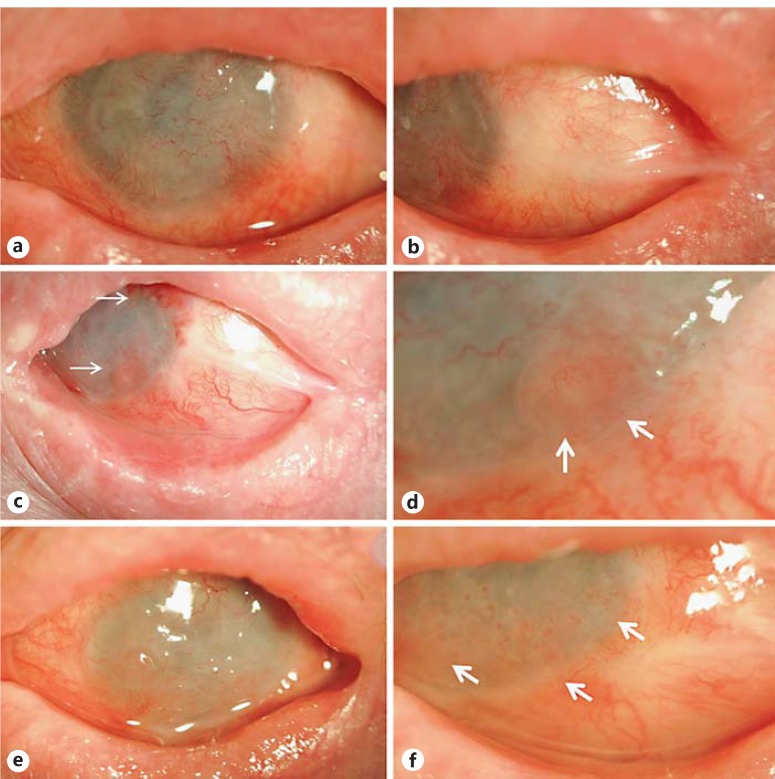
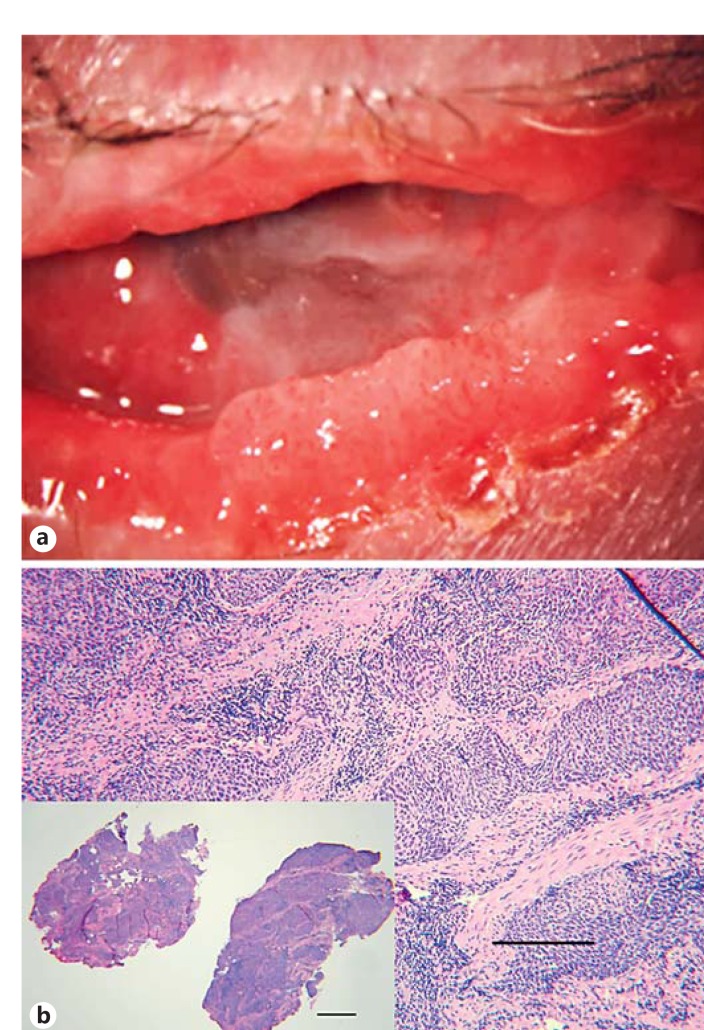
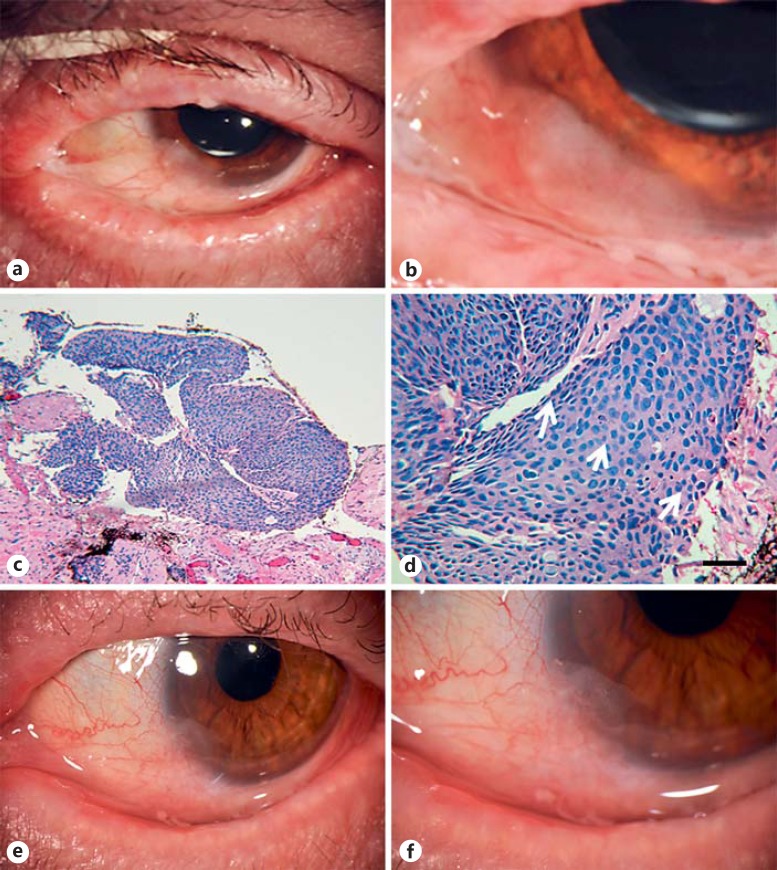
Methods: Case one involved a 73-year-old male with atopic eczema and severe AKC who developed a limbal lesion suspicious for ocular surface squamous neoplasia (OSSN). Slit-lamp examination was significant for a new sessile lesion in the temporal limbal region of the left eye. The lesion was treated with excisional biopsy and cryotherapy. Topical therapy with mitomycin C, topical interferon alpha 2b, and topical 5-fluorouracil provided only partial control. Exenteration was eventually needed. Case two involved a 53-year-old male with history of severe AKC and eczema. Computed tomography imaging showed an infiltrative mass of the right orbit. Incisional biopsies confirmed conjunctival squamous cell carcinoma of both sides (invasive in the right eye, in situ in the left eye). Exenteration was needed for control of invasive carcinoma in the right eye.
Results: Squamous cell carcinoma was treated without success in spite of surgical excision and aggressive treatment with multiple topical agents and multiple applications of cryotherapy. Orbital exenteration was needed in both cases.
Conclusion: Chronic inflammation associated with AKC may be a risk factor for the development of bilateral, diffuse, invasive, and recurrent OSSN that may require exenteration.
Keywords: Atopia; Inflammation; Masquerade; Neoplasia; Ocular surface.
Figures

References
-
- Foster CS, Calonge M. Atopic keratoconjunctivitis. Ophthalmology. 1990;97:992–1000. - PubMed
-
- Braude LS, Chandler JW. Atopic corneal disease. Int Ophthalmol Clin. 1984;24:145–156. - PubMed
-
- Tuft SJ, Kemeny DM, Dart JK, Buckley RJ. Clinical features of atopic keratoconjunctivitis. Ophthalmology. 1991;98:150–158. - PubMed
-
- Ibrahim OM, Dogru M, Kaido M, et al. Functional visual acuity assessment of severe atopic keratoconjunctivitis. Cornea. 2014;33(suppl 11):S13–S18. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
