

Impact of Calcium and Two Doses of Vitamin D on Bone Metabolism in the Elderly: A Randomized Controlled Trial
- PMID: 28276596
- PMCID: PMC5489368
- DOI: 10.1002/jbmr.3122
Impact of Calcium and Two Doses of Vitamin D on Bone Metabolism in the Elderly: A Randomized Controlled Trial
Abstract
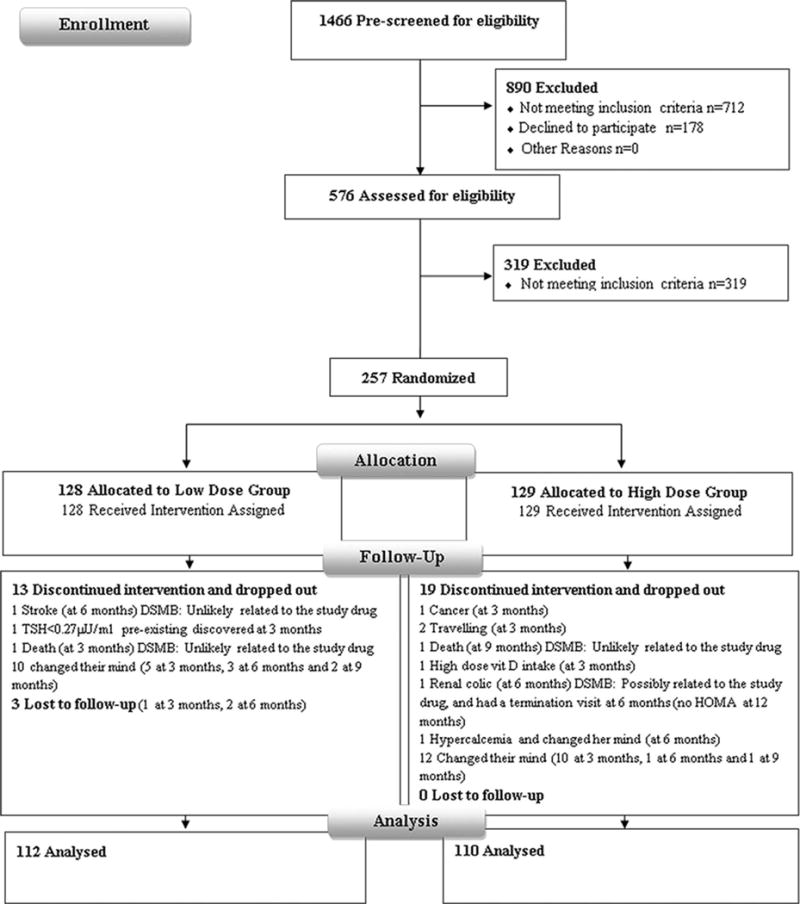
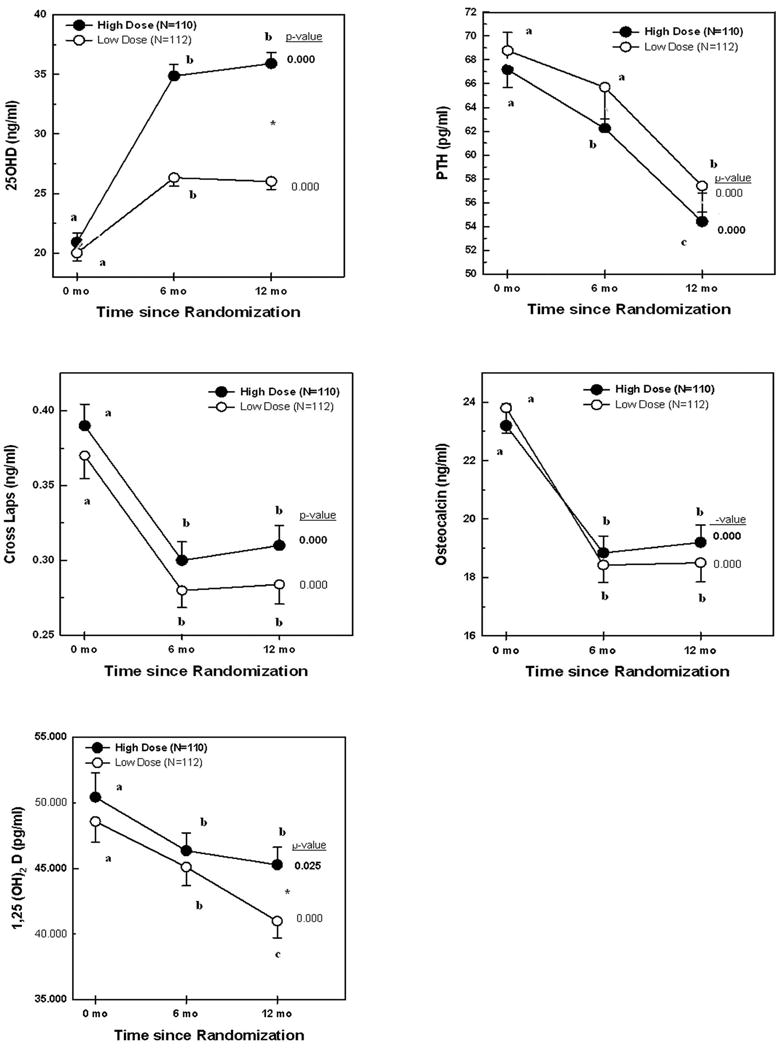
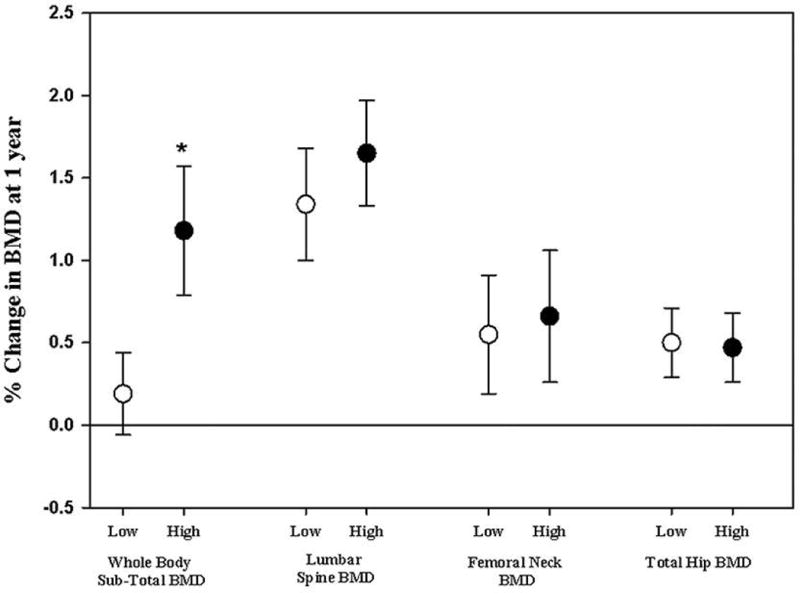
The optimal dose of vitamin D to optimize bone metabolism in the elderly is unclear. We tested the hypothesis that vitamin D, at a dose higher than recommended by the Institute of Medicine (IOM), has a beneficial effect on bone remodeling and mass. In this double-blind trial we randomized 257 overweight elderly subjects to receive 1000 mg of elemental calcium citrate/day, and the daily equivalent of 3750 IU/day or 600 IU/day of vitamin D3 for 1 year. The subjects' mean age was 71 ± 4 years, body mass index 30 ± 4 kg/m2 , 55% were women, and 222 completed the 12-month follow-up. Mean serum 25 hydroxyvitamin D (25OHD) was 20 ng/mL, and rose to 26 ng/mL in the low-dose arm, and 36 ng/mL in the high-dose arm, at 1 year (p < 0.05). Plasma parathyroid hormone, osteocalcin, and C-terminal telopeptide (Cross Laps) levels decreased significantly by 20% to 22% in both arms, but there were no differences between the two groups for any variable, at 6 or 12 months, with the exception of serum calcitriol, which was higher in the high-dose group at 12 months. Bone mineral density (BMD) increased significantly at the total hip and lumbar spine, but not the femoral neck, in both study arms, whereas subtotal body BMD increased in the high-dose group only, at 1 year. However, there were no significant differences in percent change BMD between the two study arms at any skeletal site. Subjects with serum 25OHD <20 ng/mL and PTH level >76 pg/mL showed a trend for higher BMD increments at all skeletal sites, in the high-dose group, that reached significance at the hip. Adverse events were comparable in the two study arms. This controlled trial shows little additional benefit in vitamin D supplementation at a dose exceeding the IOM recommendation of 600 IU/day on BMD and bone markers, in overweight elderly individuals. © 2017 American Society for Bone and Mineral Research.
Keywords: Elderly; IOM; bone markers; bone mineral density (BMD); high-dose vitamin D.
© 2017 American Society for Bone and Mineral Research.
Conflict of interest statement
All authors state that they have no conflict of interest
Figures
Similar articles
-
Effect of increasing doses of vitamin D on bone mineral density and serum N-terminal telopeptide in elderly women: a randomized controlled trial.J Intern Med. 2018 Dec;284(6):685-693. doi: 10.1111/joim.12825. Epub 2018 Sep 17. J Intern Med. 2018. PMID: 30137647
-
[Changes in mineral metabolism in stage 3, 4, and 5 chronic kidney disease (not on dialysis)].Nefrologia. 2008;28 Suppl 3:67-78. Nefrologia. 2008. PMID: 19018742 Spanish.
-
The effect of high-dose vitamin D supplementation on calciotropic hormones and bone mineral density in obese subjects with low levels of circulating 25-hydroxyvitamin d: results from a randomized controlled study.Calcif Tissue Int. 2013 Jul;93(1):69-77. doi: 10.1007/s00223-013-9729-3. Epub 2013 Apr 17. Calcif Tissue Int. 2013. PMID: 23591713 Clinical Trial.
-
Effect of intermittent administration of 200 IU intranasal salmon calcitonin and low doses of 1alpha(OH) vitamin D3 on bone mineral density of the lumbar spine and hip region and biochemical bone markers in women with postmenopausal osteoporosis: a pilot study.Clin Rheumatol. 2005 Jun;24(3):232-8. doi: 10.1007/s10067-004-1004-6. Epub 2005 Jan 13. Clin Rheumatol. 2005. PMID: 15647969 Clinical Trial.
-
Update on vitamin D: pros and cons.Clin Cases Miner Bone Metab. 2015 Sep-Dec;12(3):222-3. doi: 10.11138/ccmbm/2015.12.3.222. Epub 2015 Dec 29. Clin Cases Miner Bone Metab. 2015. PMID: 26811700 Free PMC article. Review.
Cited by
-
Functional Food for Elderly High in Antioxidant and Chicken Eggshell Calcium to Reduce the Risk of Osteoporosis-A Narrative Review.Foods. 2021 Mar 19;10(3):656. doi: 10.3390/foods10030656. Foods. 2021. PMID: 33808726 Free PMC article. Review.
-
Vitamin D and Calcium in Osteoporosis, and the Role of Bone Turnover Markers: A Narrative Review of Recent Data from RCTs.Diseases. 2023 Feb 8;11(1):29. doi: 10.3390/diseases11010029. Diseases. 2023. PMID: 36810543 Free PMC article.
-
A Comparison and Safety Evaluation of Micellar versus Standard Vitamin D3 Oral Supplementation in a Randomized, Double-Blind Human Pilot Study.Nutrients. 2024 May 22;16(11):1573. doi: 10.3390/nu16111573. Nutrients. 2024. PMID: 38892507 Free PMC article. Clinical Trial.
-
Scientific opinion on the tolerable upper intake level for vitamin D, including the derivation of a conversion factor for calcidiol monohydrate.EFSA J. 2023 Aug 8;21(8):e08145. doi: 10.2903/j.efsa.2023.8145. eCollection 2023 Aug. EFSA J. 2023. PMID: 37560437 Free PMC article.
-
Effect of high dose vitamin D supplementation on indices of sarcopenia and obesity assessed by DXA among older adults: A randomized controlled trial.Endocrine. 2022 Apr;76(1):162-171. doi: 10.1007/s12020-021-02951-3. Epub 2022 Jan 14. Endocrine. 2022. PMID: 35028890 Clinical Trial.
References
-
- Manson JE, Brannon PM, Rosen CJ, Taylor CL. Vitamin D Deficiency - Is There Really a Pandemic? N Engl J Med. 2016;375(19):1817–1820. - PubMed
-
- Lips P. Worldwide status of vitamin D nutrition. J Steroid Biochem Mol Biol. 2010;121(1–2):297–300. - PubMed
-
- Mithal A, Wahl DA, Bonjour JP, et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos Int. 2009;20(11):1807–20. - PubMed
-
- Wahl DA, Cooper C, Ebeling PR, et al. A global representation of vitamin D status in healthy populations. Arch Osteoporos. 2012;7:155–72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
