

Fetal growth pathology score: a novel ultrasound parameter for individualized assessment of third trimester growth abnormalities
- PMID: 28277911
- PMCID: PMC5813490
- DOI: 10.1080/14767058.2017.1300646
Fetal growth pathology score: a novel ultrasound parameter for individualized assessment of third trimester growth abnormalities
Abstract
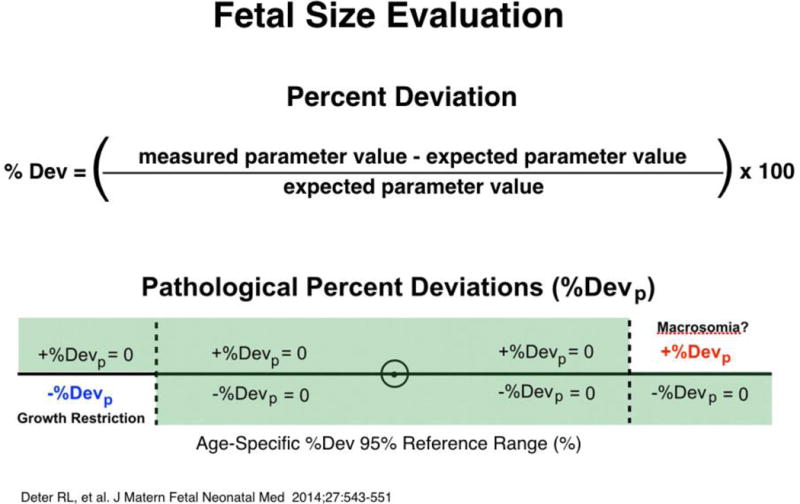
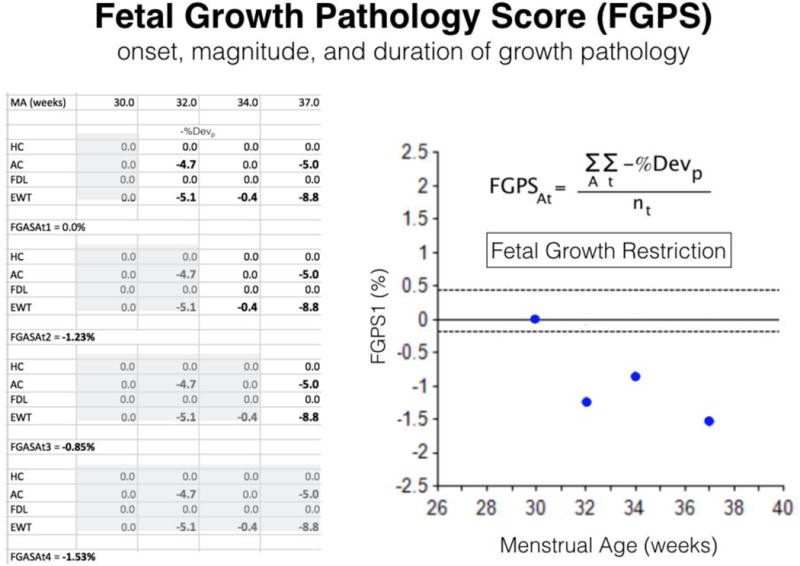
Objectives: To study fetal growth in pregnancies at risk for growth restriction (GR) using, for the first time, the fetal growth pathology score (FGPS1).
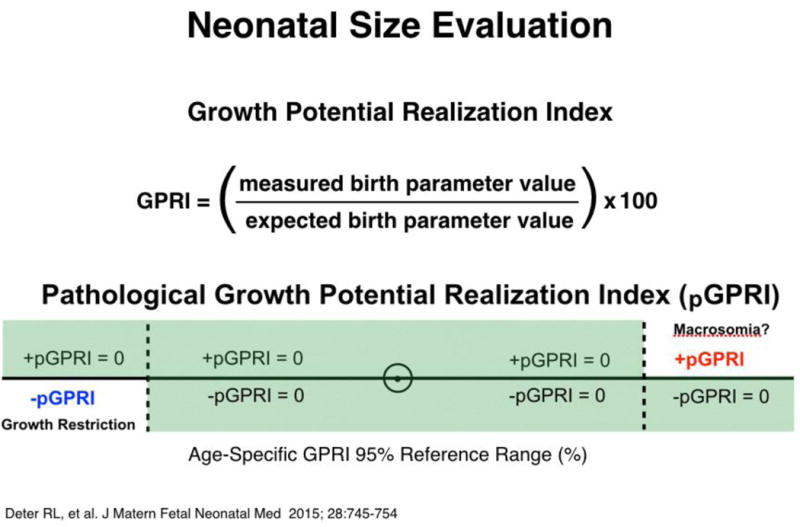
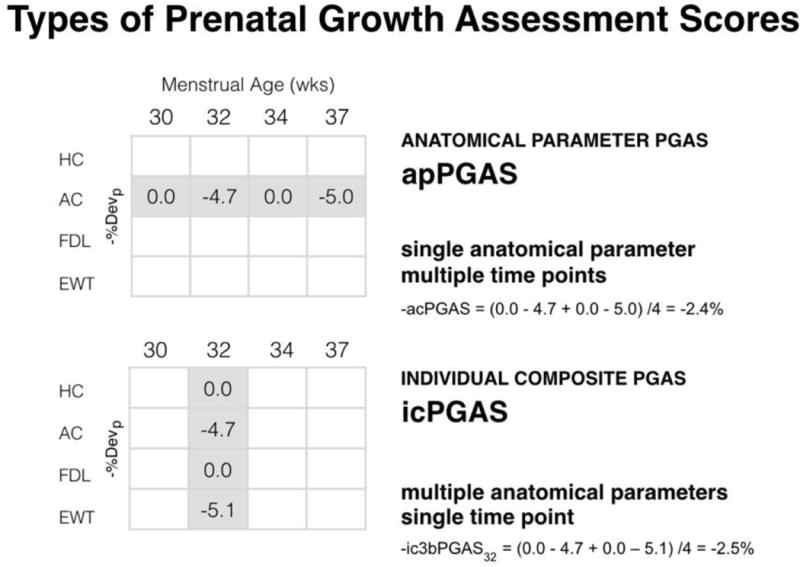
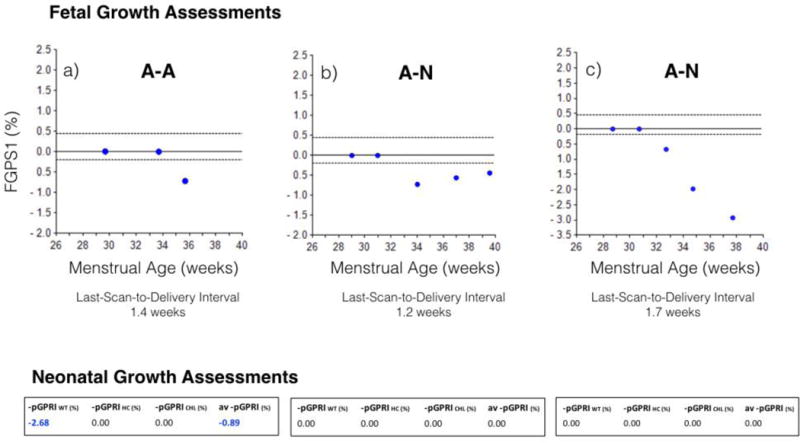
Methods: A retrospective cohort study of GR was carried out in 184 selected SGA singletons using a novel, composite measure of growth abnormalities termed the FGPS1. Serial fetal biometry was used to establish second trimester Rossavik size models and determine FGPS1 values prior to delivery. FGPS1 data were compared to neonatal growth outcomes assessed using growth potential realization index (GPRI) values (average negative pathological GPRI (av - pGPRI)). Growth at the end of pregnancy was evaluated from differences in negative, individual composite prenatal growth assessment scores (-icPGAS) measured at the last two ultrasound scans. The FGPS1 and av - pGPRI values were used to classify fetal growth and neonatal growth outcomes, respectively, as Normal (N) or Abnormal (A).
Results: The risk of neonatal GR (based on birth weight (BW)) was moderate (MR: between 5th and10th percentiles (n = 113)) or significant (SR:<5th percentile) (n = 71)). Individual pregnancies were grouped into four categories, two representing agreement (N-N (29%), A-A (40%)) and two representing discordance (N-A (11%), A-N (20%)). In the largest and most variable subgroup (A-A,<5%tile, n = 49), there was a statistically significant correlation (0.63, p < .0001) between the FGPS1 and av - pGPRI. In N-A, all 20 cases (100%) had long last-scan-to-delivery intervals (1.9 weeks or greater), suggesting late development of the growth abnormality. For A-N, in approximately equal proportions, GR was improving, progressing or unclassifiable at the end of pregnancy.
Conclusions: Significant agreement between prenatal and postnatal growth assessments was found using a novel approach for quantifying fetal growth pathology (FGPS1). Discordances appear to be due to lack of appropriate prenatal scans or an inadequate set of neonatal measurements. Evidence for a quantitative relationship between assessment methods was seen in the largest and most variable subgroup. The FGPS1 has the potential for characterizing GR in the third trimester and may provide a means for predicting the severity of corresponding abnormal neonatal growth outcomes.
Keywords: Individualized growth assessment; SGA; longitudinal growth study.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Third-trimester growth diversity in small fetuses classified as appropriate-for-gestational age or small-for-gestational age at birth.Ultrasound Obstet Gynecol. 2021 Dec;58(6):882-891. doi: 10.1002/uog.23688. Ultrasound Obstet Gynecol. 2021. PMID: 33998089
-
Can growth in dichorionic twins be monitored with individualized growth assessment?Ultrasound Obstet Gynecol. 2023 Dec;62(6):829-835. doi: 10.1002/uog.26320. Ultrasound Obstet Gynecol. 2023. PMID: 37488689
-
Growth patterns and cardiovascular abnormalities in SGA fetuses: 2. Normal growth and progressive growth restriction.J Matern Fetal Neonatal Med. 2022 Jul;35(14):2818-2827. doi: 10.1080/14767058.2020.1807506. Epub 2020 Sep 13. J Matern Fetal Neonatal Med. 2022. PMID: 32924675
-
The World Health Organization fetal growth charts: concept, findings, interpretation, and application.Am J Obstet Gynecol. 2018 Feb;218(2S):S619-S629. doi: 10.1016/j.ajog.2017.12.010. Am J Obstet Gynecol. 2018. PMID: 29422204 Review.
-
Fetal growth velocity and body proportion in the assessment of growth.Am J Obstet Gynecol. 2018 Feb;218(2S):S700-S711.e1. doi: 10.1016/j.ajog.2017.12.014. Am J Obstet Gynecol. 2018. PMID: 29422209 Review.
Cited by
-
Intrauterine Growth Restriction: New Insight from the Metabolomic Approach.Metabolites. 2019 Nov 6;9(11):267. doi: 10.3390/metabo9110267. Metabolites. 2019. PMID: 31698738 Free PMC article. Review.
-
Second trimester growth velocities: assessment of fetal growth potential in SGA singletons.J Matern Fetal Neonatal Med. 2019 Mar;32(6):939-946. doi: 10.1080/14767058.2017.1395849. Epub 2017 Nov 7. J Matern Fetal Neonatal Med. 2019. PMID: 29057683 Free PMC article.
-
Fractional fetal thigh volume in the prediction of normal and abnormal fetal growth during the third trimester of pregnancy.Am J Obstet Gynecol. 2017 Oct;217(4):453.e1-453.e12. doi: 10.1016/j.ajog.2017.06.018. Epub 2017 Jun 23. Am J Obstet Gynecol. 2017. PMID: 28651860 Free PMC article.
-
Fetal Growth Restriction - Diagnostic Work-up, Management and Delivery.Geburtshilfe Frauenheilkd. 2020 Oct;80(10):1016-1025. doi: 10.1055/a-1232-1418. Epub 2020 Sep 25. Geburtshilfe Frauenheilkd. 2020. PMID: 33012833 Free PMC article.
-
Third trimester growth restriction patterns: individualized assessment using a fetal growth pathology score.J Matern Fetal Neonatal Med. 2018 Aug;31(16):2155-2163. doi: 10.1080/14767058.2017.1337741. Epub 2017 Jul 6. J Matern Fetal Neonatal Med. 2018. PMID: 28573931 Free PMC article.
References
-
- American College of Obstetricians and Gynecologists. ACOG Practice bulletin no. 134: fetal growth restriction. Obstet Gynecol. 2013;121:1122–33. - PubMed
-
- Sharma D, Farahbakhsh N, Shastri S, Sharma P. Intrauterine growth restriction - part 2. J Matern Fetal Neonatal Med. 2016;11:1–12.
-
- Villar J, Ismail LE, Victora CG, et al. International standards for newborn weight, length and head circumference by gestational age and sex: the newborn cross-sectional study of the INTERGROWTH-21st project. Lancet. 2014;384:857–68. - PubMed
-
- Papageorghiou AT, Ohuma EO, Altman DG, et al. International standards for fetal growth based on serial ultrasound measurements: the fetal growth longitudinal study of the INTERGROWTH-21st project. Lancet. 2014;384:869–79. - PubMed
-
- Deter RL. Individualized growth assessment: evaluation of growth using each fetus as its own control. Semin Perinatol. 2004;28:23–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials