

Diagnostic Efficiency of the Child and Adolescent Symptom Inventory (CASI-4R) Depression Subscale for Identifying Youth Mood Disorders
- PMID: 28278596
- PMCID: PMC5801256
- DOI: 10.1080/15374416.2017.1280807
Diagnostic Efficiency of the Child and Adolescent Symptom Inventory (CASI-4R) Depression Subscale for Identifying Youth Mood Disorders
Abstract
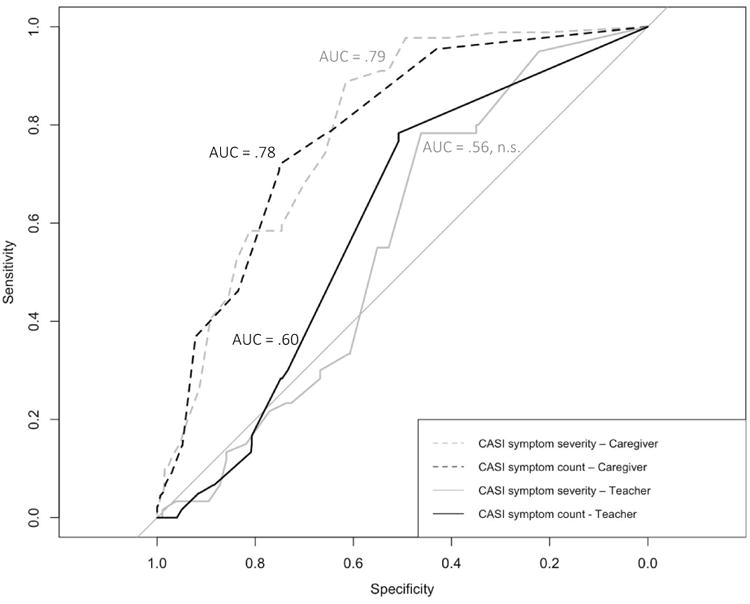
This study examined the diagnostic and clinical utility of the Child and Adolescent Symptom Inventory-4 R (CASI-4 R) Depressive and Dysthymia subscale for detecting mood disorders in youth (ages 6-12; M = 9.37) visiting outpatient mental health clinics. Secondary analyses (N = 700) utilized baseline data from the Longitudinal Assessment of Manic Symptoms study. Semistructured interviews with youth participants and their parents/caregivers determined psychiatric diagnoses. Caregivers and teachers completed the CASI-4 R. CASI-4 R depressive symptom severity and symptom count scores each predicted mood disorder diagnoses. Both caregiver scores (symptom severity and symptom count) of the CASI-4 R subscale significantly identified youth mood disorders (areas under the curve [AUCs] = .78-.79, ps < .001). The symptom severity version showed a small but significant advantage. Teacher symptom severity report did not significantly predict mood disorder diagnosis (AUC = .56, p > .05), whereas the teacher symptom count report corresponded to a small effect size (AUC = .61, p < .05). The CASI-4 R Depression scale showed strong incrememental validity even controlling for the other CASI-4 R scales. Caregiver subscale cutoff scores were calculated to assist in ruling in (diagnostic likelihood ratio [DLR] = 3.73) or ruling out (DLR = 0.18) presence of a mood disorder. The CASI-4 R Depressive subscale caregiver report can help identify youth mood disorders, and using DLRs may help improve diagnostic accuracy.
Figures
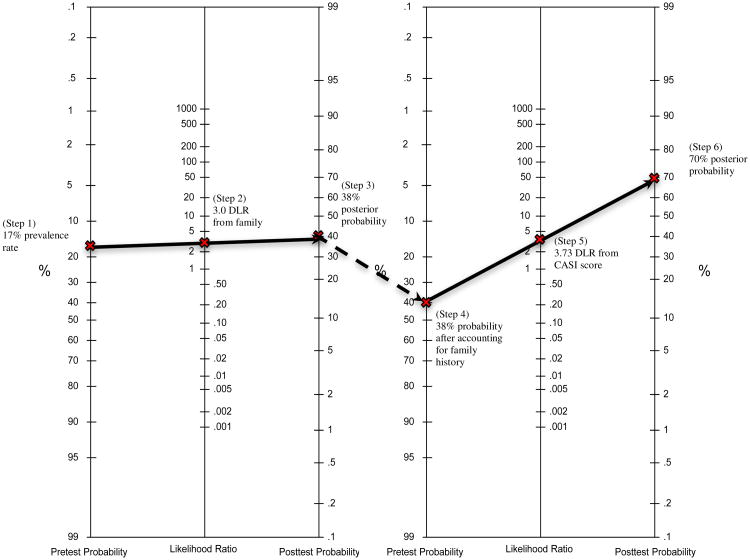
Select the pretest probability and plot it on the first line on the left side of the nomogram. In this example, we use 17% as the base rate of depressive disorders in an outpatient clinic.
Determine and plot the diagnostic likelihood ratio (DLR) associated with the risk factor on the second line. For instance, we found that depression in parents is associated with a three-fold increase in risk for developing major depression (DLR = 3.0; Weissman et al., 2006).
Connect the dots and extend the line to the third line to determine that the posttest probability estimate is 38%.
To incorporate additional information, repeat the process using the posttest probability as the new pretest probability estimate in the second nomogram.
Plot the DLR associated with the parent's CASI depression severity score; in this example, a score of 17 corresponds to a DLR of 3.73 (see Table 3).
Connect the dots to determine the new posttest probability estimate of 70%.
References
-
- Achenbach TM, Rescorla LA. Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont; 2001.
-
- Ægisdóttir S, White MJ, Spengler PM, Maugherman AS, Anderson LA, Cook RS, et al. Cohen G. The meta-analysis of clinical judgment project: Fifty-six years of accumulated research on clinical versus statistical prediction. The Counseling Psychologist. 2006;34(3):341–382. doi: 10.1177/0011000005285875. - DOI
-
- American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th. Arlington, VA: American Psychiatric Publishing, Inc; 2013.
-
- Bayes T, Price R. An Essay towards solving a Problem in the Doctrine of Chances. By the late Rev. Mr. Bayes, communicated by Mr. Price, in a letter to John Canton, M. A. and F. R. S. Philosophical Transactions of the Royal Society of London (1683-1775) 1763;53:370–418.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical