

ICARES: a real-time automated detection tool for clusters of infectious diseases in the Netherlands
- PMID: 28279150
- PMCID: PMC5345172
- DOI: 10.1186/s12879-017-2300-5
ICARES: a real-time automated detection tool for clusters of infectious diseases in the Netherlands
Abstract
Background: Clusters of infectious diseases are frequently detected late. Real-time, detailed information about an evolving cluster and possible associated conditions is essential for local policy makers, travelers planning to visit the area, and the local population. This is currently illustrated in the Zika virus outbreak.
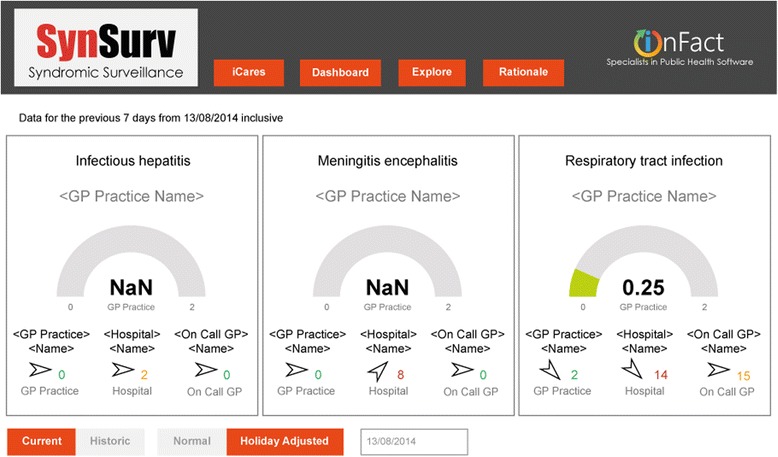
Methods: In the Netherlands, ICARES (Integrated Crisis Alert and Response System) has been developed and tested on three syndromes as an automated, real-time tool for early detection of clusters of infectious diseases. From local general practices, General Practice Out-of-Hours services and a hospital, the numbers of routinely used syndrome codes for three piloted tracts i.e., respiratory tract infection, hepatitis and encephalitis/meningitis, are sent on a daily basis to a central unit of infectious disease control. Historic data combined with information about patients' syndromes, age cohort, gender and postal code area have been used to detect clusters of cases.
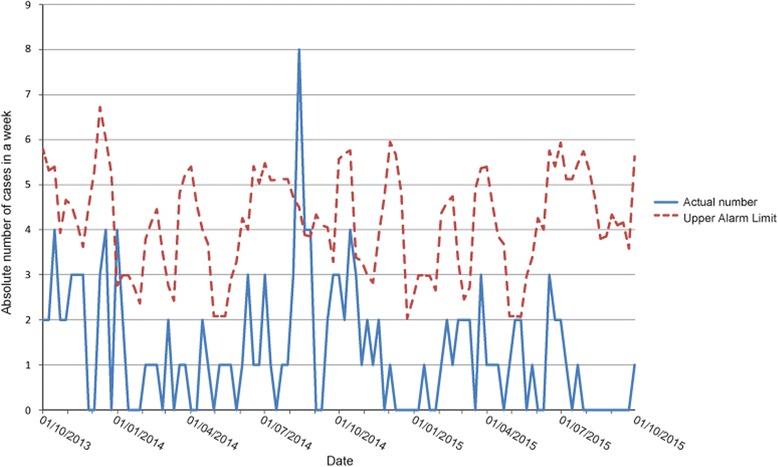
Results: During the first 2 years, two out of eight alerts appeared to be a real cluster. The first was part of the seasonal increase in Enterovirus encephalitis and the second was a remarkably long lasting influenza season with high peak incidence.
Conclusions: This tool is believed to be the first flexible automated, real-time cluster detection system for infectious diseases, based on physician information from both general practitioners and hospitals. ICARES is able to detect and follow small regional clusters in real time and can handle any diseases entity that is regularly registered by first line physicians. Its value will be improved when more health care institutions agree to link up with ICARES thus improving further the signal-to-noise ratio.
Keywords: Automated; Cluster detection; Hepatitis; Meningoencephalitis; Real-time; Respiratory tract infection.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
