

Receiver operating characteristic analysis of prediction for gastric cancer development using serum pepsinogen and Helicobacter pylori antibody tests
- PMID: 28279154
- PMCID: PMC5345231
- DOI: 10.1186/s12885-017-3173-0
Receiver operating characteristic analysis of prediction for gastric cancer development using serum pepsinogen and Helicobacter pylori antibody tests
Abstract
Background: Chronic Helicobacter pylori infection plays a central role in the development of gastric cancer as shown by biological and epidemiological studies. The H. pylori antibody and serum pepsinogen (PG) tests have been anticipated to predict gastric cancer development.
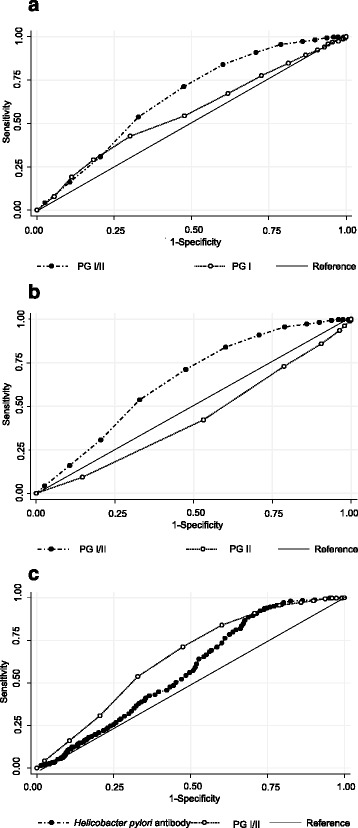
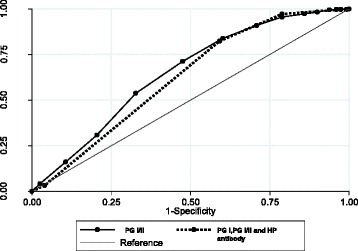
Methods: We determined the predictive sensitivity and specificity of gastric cancer development using these tests. Receiver operating characteristic analysis was performed, and areas under the curve were estimated. The predictive sensitivity and specificity of gastric cancer development were compared among single tests and combined methods using serum pepsinogen and H. pylori antibody tests.
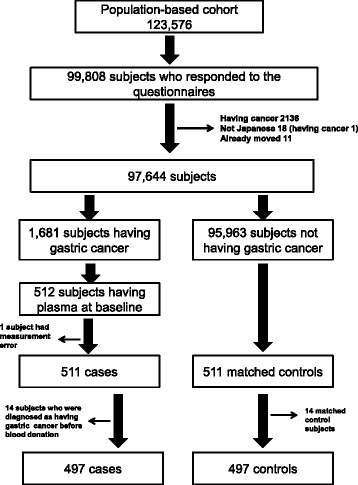
Results: From a large-scale population-based cohort of over 100,000 subjects followed between 1990 and 2004, 497 gastric cancer subjects and 497 matched healthy controls were chosen. The predictive sensitivity and specificity were low in all single tests and combination methods. The highest predictive sensitivity and specificity were obtained for the serum PG I/II ratio. The optimal PG I/II cut-off values were 2.5 and 3.0. At a PG I/II cut-off value of 3.0, the sensitivity was 86.9% and the specificity was 39.8%. Even if three biomarkers were combined, the sensitivity was 97.2% and the specificity was 21.1% when the cut-off values were 3.0 for PG I/II, 70 ng/mL for PG I, and 10.0 U/mL for H. pylori antibody.
Conclusions: The predictive accuracy of gastric cancer development was low with the serum pepsinogen and H. pylori antibody tests even if these tests were combined. To adopt these biomarkers for gastric cancer screening, a high specificity is required. When these tests are adopted for gastric cancer screening, they should be carefully interpreted with a clear understanding of their limitations.
Keywords: Cancer screening; Gastric cancer; Helicobacter pylori antibody; Receiver operating characteristic analysis; Serum pepsinogen.
Figures
References
-
- International Agency for Research on Cancer: GLOBOCAN. 2012. http://globocan.iarc.fr/. Accessed 10 Aug 2016.
-
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans . IARC Working Group Reports Volume 8. Helicobacter pylori eradication as a strategy for preventing gastric cancer. Lyon: IARC; 2014. HELICOBACTER PYLORI; pp. 1–4.
-
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans . HELICOBACTER PYLORI. In: International Agency of Research on Cancer. IARC Monographs on the evaluation of carcinogenic risks to human: Biological agents. Volume 100B. Lyon: IARC; 2012. pp. 385–435.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
