

Effect of a standardized treatment regime for infection after osteosynthesis
- PMID: 28279223
- PMCID: PMC5345171
- DOI: 10.1186/s13018-017-0535-x
Effect of a standardized treatment regime for infection after osteosynthesis
Abstract
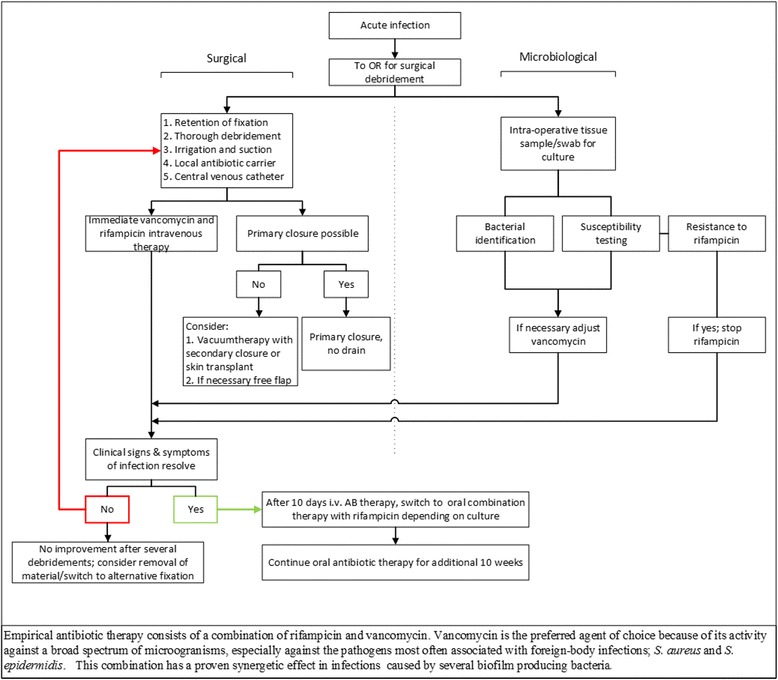
Background: Infection after osteosynthesis is an important complication with significant morbidity and even mortality. These infections are often caused by biofilm-producing bacteria. Treatment algorithms dictate an aggressive approach with surgical debridement and antibiotic treatment. The aim of this study is to analyze the effect of such an aggressive standardized treatment regime with implant retention for acute, existing <3 weeks, infection after osteosynthesis.
Methods: We conducted a retrospective 2-year cohort in a single, level 1 trauma center on infection occurring within 12 months following any osteosynthesis surgery. The standardized treatment regime consisted of implant retention, thorough surgical debridement, and immediate antibiotic combination therapy with rifampicin. The primary outcome was success. Success was defined as consolidation of the fracture and resolved symptoms of infection. Culture and susceptibility testing were performed to identify bacteria and resistance patterns. Univariate analysis was conducted on patient-related factors in association with primary success and antibiotic resistance.
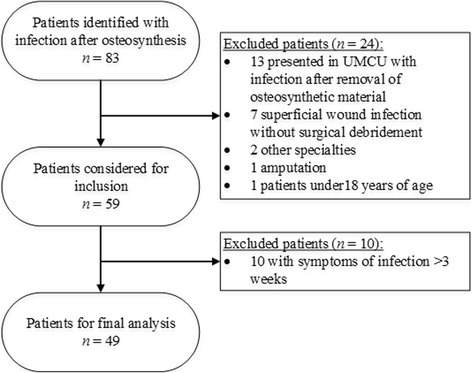
Results: Forty-nine patients were included for analysis. The primary success rate was 63% and overall success rate 88%. Factors negatively associated with primary success were the following: Gustilo classification (P = 0.023), higher number of debridements needed (P = 0.015), inability of primary closure (P = 0.017), and subsequent application of vacuum therapy (P = 0.030). Adherence to the treatment regime was positively related to primary success (P = 0.034).
Conclusions: The described treatment protocol results in high success rates, comparable with success rates achieved in staged exchange in prosthetic joint infection treatment.
Keywords: Fracture; Infection; ORIF; Osteomyelitis; Osteosynthesis; Treatment.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
