

Doxycycline versus prednisolone as an initial treatment strategy for bullous pemphigoid: a pragmatic, non-inferiority, randomised controlled trial
- PMID: 28279484
- PMCID: PMC5400809
- DOI: 10.1016/S0140-6736(17)30560-3
Doxycycline versus prednisolone as an initial treatment strategy for bullous pemphigoid: a pragmatic, non-inferiority, randomised controlled trial
Erratum in
-
Department of Error.Lancet. 2017 Oct 28;390(10106):1948. doi: 10.1016/S0140-6736(17)32703-4. Epub 2017 Oct 26. Lancet. 2017. PMID: 29115227 Free PMC article. No abstract available.
Abstract
Background: Bullous pemphigoid is a blistering skin disorder with increased mortality. We tested whether a strategy of starting treatment with doxycycline gives acceptable short-term blister control while conferring long-term safety advantages over starting treatment with oral corticosteroids.
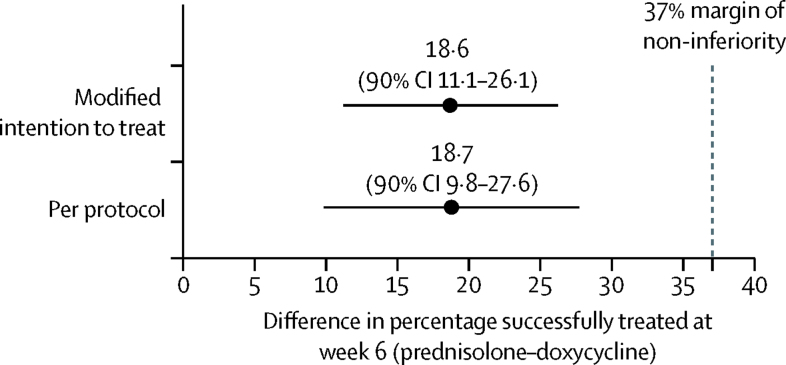
Methods: We did a pragmatic, multicentre, parallel-group randomised controlled trial of adults with bullous pemphigoid (three or more blisters at two or more sites and linear basement membrane IgG or C3). Participants were randomly assigned to doxycycline (200 mg per day) or prednisolone (0·5 mg/kg per day) using random permuted blocks of randomly varying size, and stratified by baseline severity (3-9, 10-30, and >30 blisters for mild, moderate, and severe disease, respectively). Localised adjuvant potent topical corticosteroids (<30 g per week) were permitted during weeks 1-3. The non-inferiority primary effectiveness outcome was the proportion of participants with three or fewer blisters at 6 weeks. We assumed that doxycycline would be 25% less effective than corticosteroids with a 37% acceptable margin of non-inferiority. The primary safety outcome was the proportion with severe, life-threatening, or fatal (grade 3-5) treatment-related adverse events by 52 weeks. Analysis (modified intention to treat [mITT] for the superiority safety analysis and mITT and per protocol for non-inferiority effectiveness analysis) used a regression model adjusting for baseline disease severity, age, and Karnofsky score, with missing data imputed. The trial is registered at ISRCTN, number ISRCTN13704604.
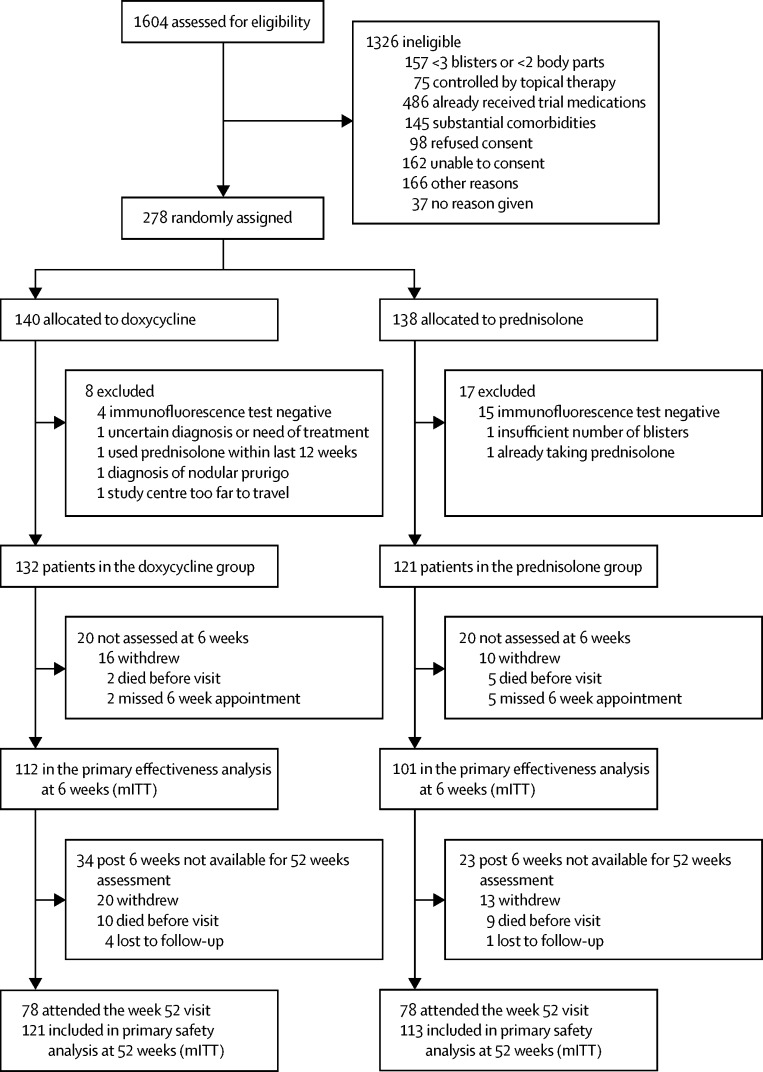
Findings: Between March 1, 2009, and Oct 31, 2013, 132 patients were randomly assigned to doxycycline and 121 to prednisolone from 54 UK and seven German dermatology centres. Mean age was 77·7 years (SD 9·7) and 173 (68%) of 253 patients had moderate-to-severe baseline disease. For those starting doxycycline, 83 (74%) of 112 patients had three or fewer blisters at 6 weeks compared with 92 (91%) of 101 patients on prednisolone, an adjusted difference of 18·6% (90% CI 11·1-26·1) favouring prednisolone (upper limit of 90% CI, 26·1%, within the predefined 37% margin). Related severe, life-threatening, and fatal events at 52 weeks were 18% (22 of 121) for those starting doxycycline and 36% (41 of 113) for prednisolone (mITT), an adjusted difference of 19·0% (95% CI 7·9-30·1), p=0·001.
Interpretation: Starting patients on doxycycline is non-inferior to standard treatment with oral prednisolone for short-term blister control in bullous pemphigoid and significantly safer in the long-term.
Funding: NIHR Health Technology Assessment Programme.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Doxycycline: a first-line treatment for bullous pemphigoid?Lancet. 2017 Apr 22;389(10079):1586-1588. doi: 10.1016/S0140-6736(17)30549-4. Epub 2017 Mar 6. Lancet. 2017. PMID: 28279483 No abstract available.
-
The BLISTER study: possible overestimation of tetracycline efficacy.Lancet. 2017 Aug 19;390(10096):735. doi: 10.1016/S0140-6736(17)31808-1. Lancet. 2017. PMID: 28831989 No abstract available.
-
Doxycycline and the treatment for bullous pemphigoid: what outcomes are most important to our patients?Br J Dermatol. 2017 Nov;177(5):1145-1147. doi: 10.1111/bjd.15890. Br J Dermatol. 2017. PMID: 29192991 No abstract available.
References
-
- Schmidt E, Zillikens D. Pemphigoid diseases. Lancet. 2013;381:320–332. - PubMed
-
- Joly P, Roujeau JC, Benichou J. A comparison of two regimens of topical corticosteroids in the treatment of patients with bullous pemphigoid: a multicenter randomized study. J Invest Dermatol. 2009;129:1681–1687. - PubMed
-
- Lever WF. Pemphigus. Medicine (Baltimore) 1953;32:1–123. - PubMed
-
- Joly P, Baricault S, Sparsa A. Incidence and mortality of bullous pemphigoid in France. J Invest Dermatol. 2012;132:1998–2004. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
