

High mortality after ALPPS for perihilar cholangiocarcinoma: case-control analysis including the first series from the international ALPPS registry
- PMID: 28279621
- PMCID: PMC5662942
- DOI: 10.1016/j.hpb.2016.10.008
High mortality after ALPPS for perihilar cholangiocarcinoma: case-control analysis including the first series from the international ALPPS registry
Abstract
Introduction: Resection of perihilar cholangiocarcinoma (PHC) entails high-risk surgery with postoperative mortality reported up to 18%, even in specialized centers. The aim of this study was to compare outcomes of PHC patients who underwent associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) to patients who underwent resection without ALPPS.
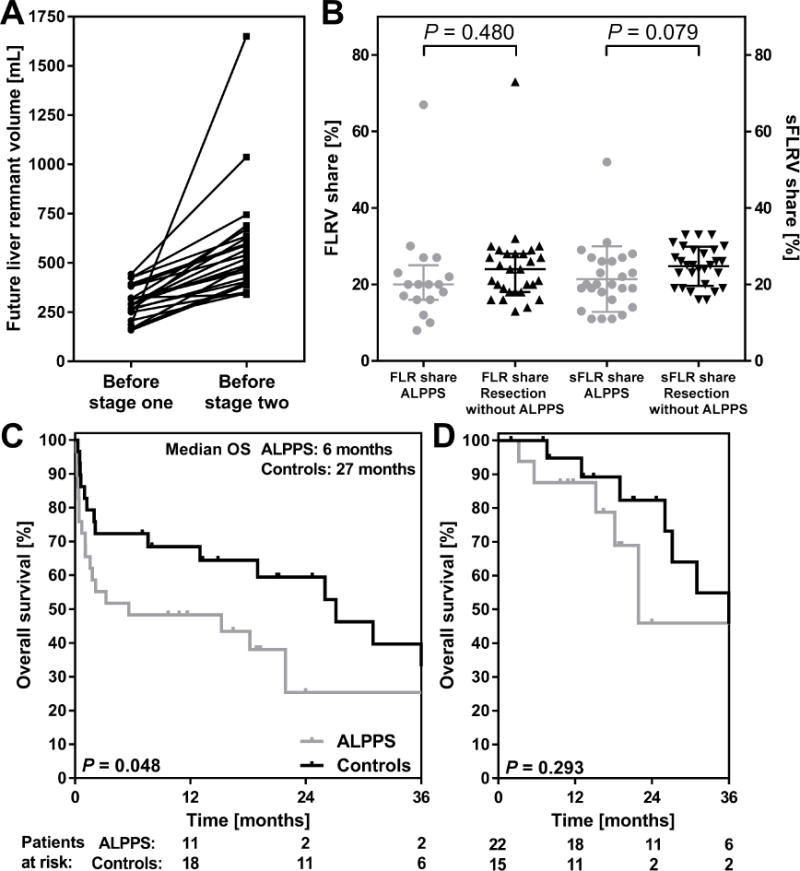
Methods: All patients who underwent ALPPS for PHC were identified from the international ALPPS registry and matched controls were selected from a standard resection cohort from two centers based on future remnant liver size. Outcomes included morbidity, mortality, and overall survival.
Results: ALPPS for PHC was associated with 48% (14/29) 90-day mortality. 90-day mortality was 13% in 257 patients who underwent major liver resection for PHC without ALPPS. The 29 ALPPS patients were matched to 29 patients resected without ALPPS, with similar future liver remnant volume (P = 0.480). Mortality in the matched control group was 24% (P = 0.100) and median OS was 27 months, comparted to 6 months after ALPPS (P = 0.064).
Discussion: Outcomes of ALPPS for PHC appear inferior compared to standard extended resections in high-risk patients. Therefore, portal vein embolization should remain the preferred method to increase future remnant liver volume in patients with PHC. ALPPS is not recommended for PHC.
Copyright © 2016. Published by Elsevier Ltd.
Figures
Comment in
-
Outcome of ALPPS for perihilar cholangiocarcinoma: case-control analysis including the first series from the international ALPPS registry.HPB (Oxford). 2017 May;19(5):379-380. doi: 10.1016/j.hpb.2017.01.024. Epub 2017 Mar 3. HPB (Oxford). 2017. PMID: 28262523 No abstract available.
References
-
- Nagino M, Ebata T, Yokoyama Y, Igami T, Sugawara G, Takahashi Y, et al. Evolution of surgical treatment for perihilar cholangiocarcinoma: a single-center 34-year review of 574 consecutive resections. Ann Surg. 2013;258(1):129–40. - PubMed
-
- Khan SA, Davidson BR, Goldin RD, Heaton N, Karani J, Pereira SP, et al. Guidelines for the diagnosis and treatment of cholangiocarcinoma: an update. Gut. 2012;61(12):1657–69. - PubMed
-
- Yokoyama Y, Nagino M, Nimura Y. Mechanism of impaired hepatic regeneration in cholestatic liver. J Hepatobiliary Pancreat Surg. 2007;14(2):159–66. - PubMed
-
- Belghiti J, Hiramatsu K, Benoist S, Massault P, Sauvanet A, Farges O. Seven hundred forty-seven hepatectomies in the 1990s: an update to evaluate the actual risk of liver resection. J Am Coll Surg. 2000;191(1):38–46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
