

Newly Formed Reticulated Platelets Undermine Pharmacokinetically Short-Lived Antiplatelet Therapies
- PMID: 28279968
- PMCID: PMC5405774
- DOI: 10.1161/ATVBAHA.116.308763
Newly Formed Reticulated Platelets Undermine Pharmacokinetically Short-Lived Antiplatelet Therapies
Abstract
Objective: Aspirin together with thienopyridine P2Y12 inhibitors, commonly clopidogrel, is a cornerstone of antiplatelet therapy. However, many patients receiving this therapy display high on-treatment platelet reactivity, which is a major therapeutic hurdle to the prevention of recurrent thrombotic events. The emergence of uninhibited platelets after thrombopoiesis has been proposed as a contributing factor to high on-treatment platelet reactivity. Here, we investigate the influences of platelet turnover on platelet aggregation in the face of different dual-antiplatelet therapy strategies.
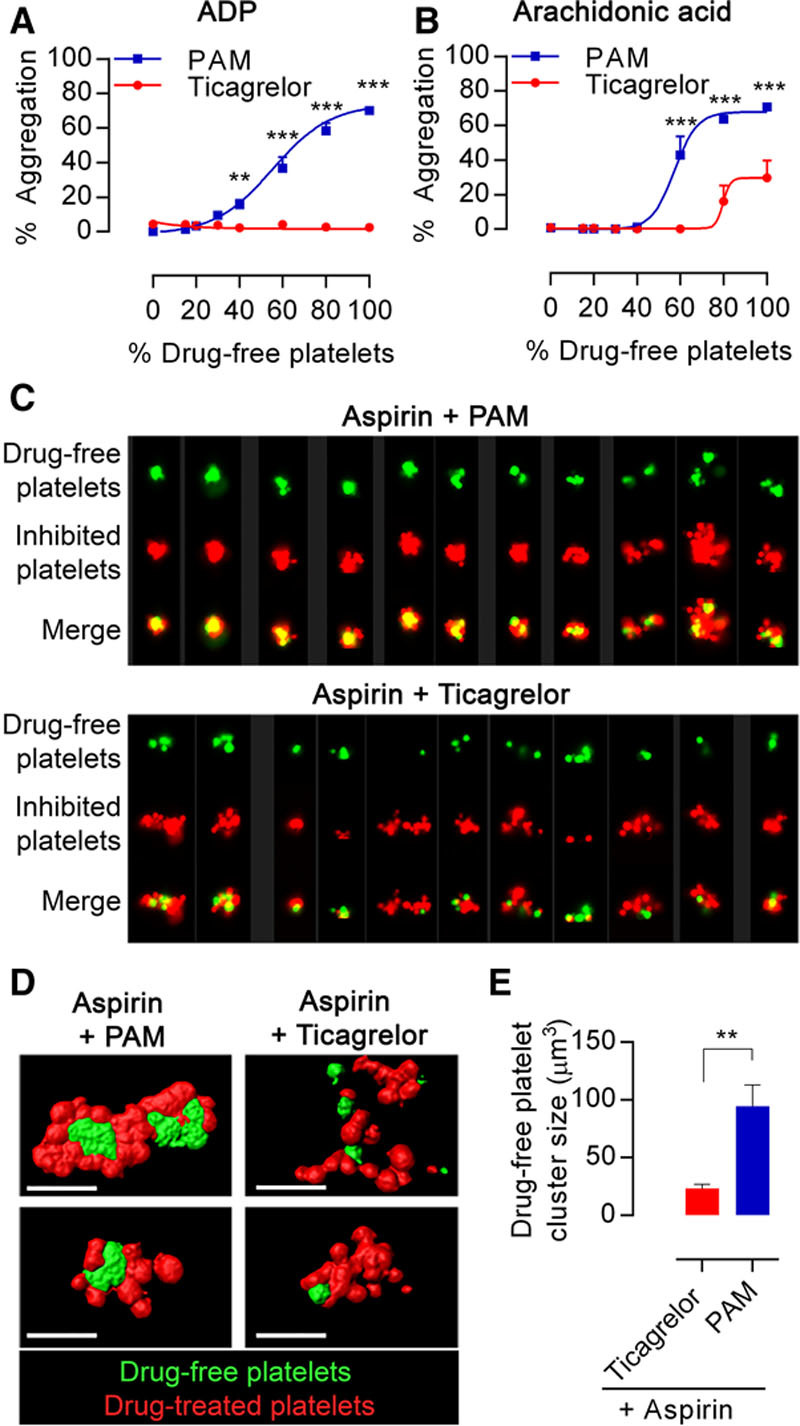
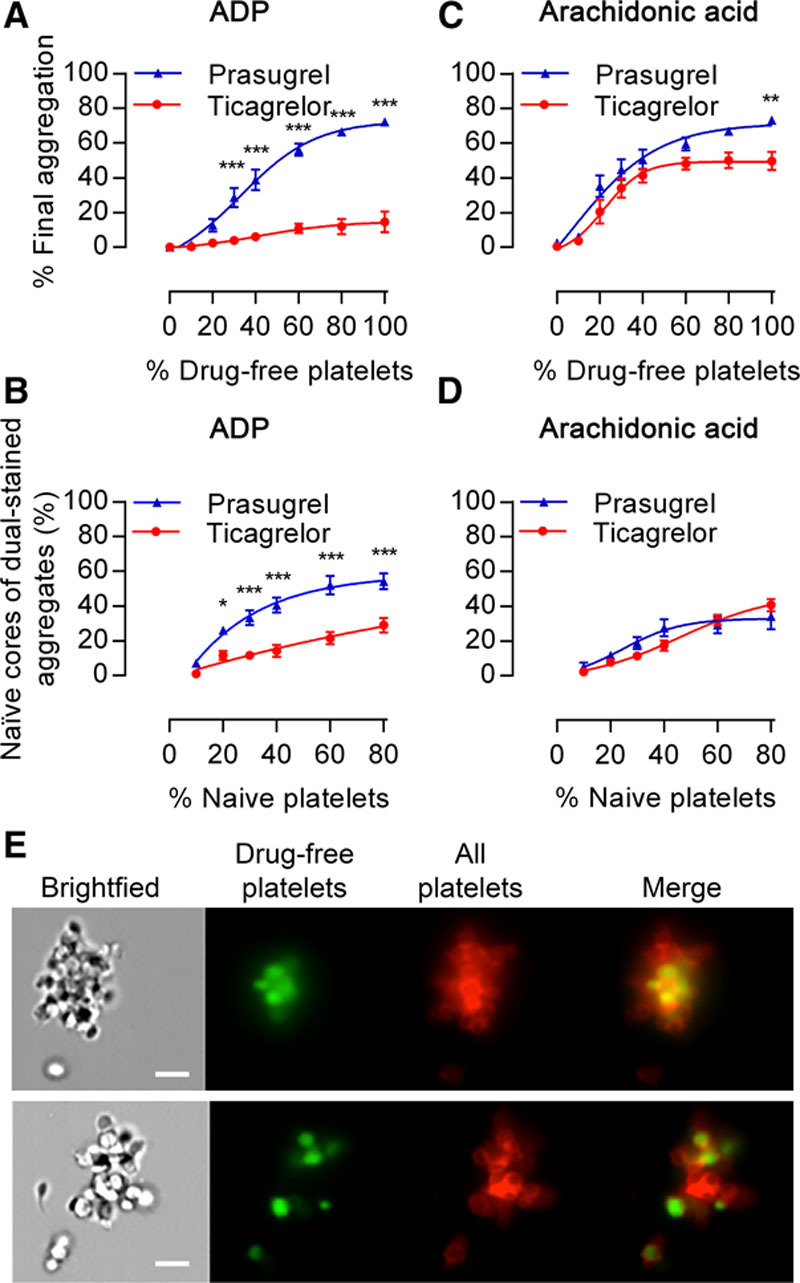
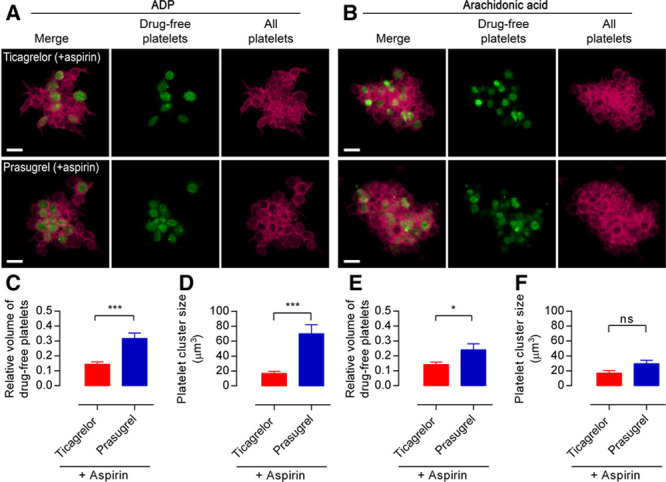
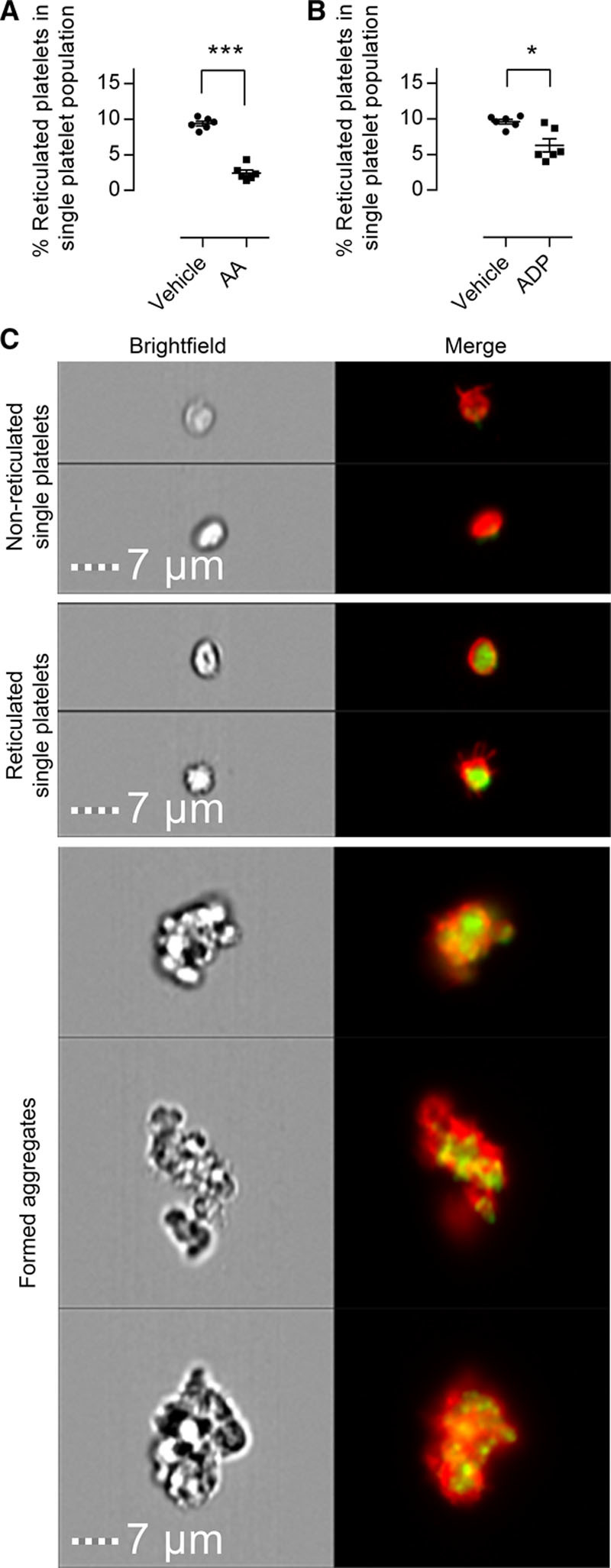
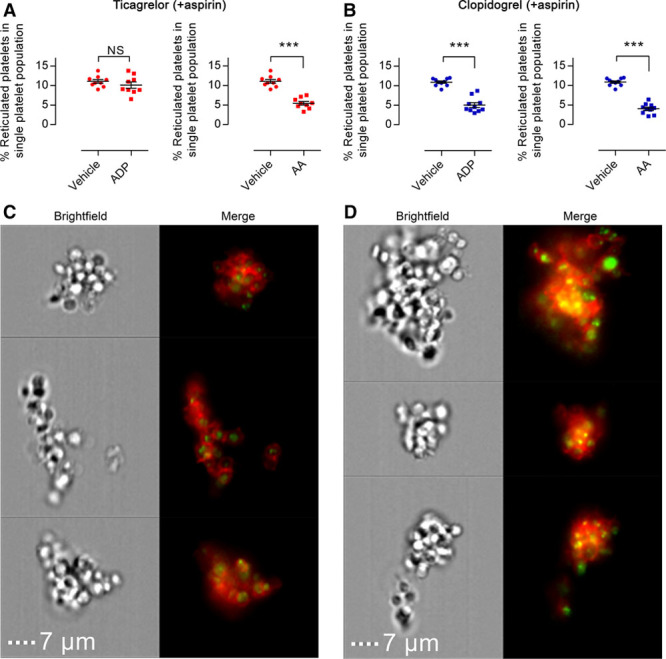
Approach and results: Traditional light transmission aggregometry, cytometry, advanced flow cytometric imaging, and confocal microscopy were used to follow the interactions of populations of platelets from healthy volunteers and patients with stable cardiovascular disease. Newly formed, reticulated platelets overproportionately contributed to, and clustered at, the core of forming aggregates. This phenomenon was particularly observed in samples from patients treated with aspirin plus a thienopyridine, but was absent in samples taken from patients treated with aspirin plus ticagrelor.
Conclusions: Reticulated platelets are more reactive than older platelets and act as seeds for the formation of platelet aggregates even in the presence of antiplatelet therapy. This is coherent with the emergence of an uninhibited subpopulation of reticulated platelets during treatment with aspirin plus thienopyridine, explained by the short pharmacokinetic half-lives of these drugs. This phenomenon is absent during treatment with ticagrelor, because of its longer half-life and ability to act as a circulating inhibitor. These data highlight the important influences of pharmacokinetics on antiplatelet drug efficacies, especially in diseases associated with increased platelet turnover.
Keywords: aspirin; blood platelets; platelet aggregation; thienopyridines; thrombosis.
© 2017 The Authors.
Figures
References
-
- Mehta SR, Yusuf S, Peters RJ, Bertrand ME, Lewis BS, Natarajan MK, Malmberg K, Rupprecht H, Zhao F, Chrolavicius S, Copland I, Fox KA Clopidogrel in Unstable angina to prevent Recurrent Events trial (CURE) Investigators. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet. 2001;358:527–533. - PubMed
-
- Tantry US, Gurbel PA. Antiplatelet drug resistance and variability in response: the role of antiplatelet therapy monitoring. Curr Pharm Des. 2013;19:3795–3815. - PubMed
-
- Tantry US, Bonello L, Aradi D, et al. Working Group on On-Treatment Platelet Reactivity. Consensus and update on the definition of on-treatment platelet reactivity to adenosine diphosphate associated with ischemia and bleeding. J Am Coll Cardiol. 2013;62:2261–2273. doi: 10.1016/j.jacc.2013.07.101. - PubMed
-
- Reny JL, Fontana P, Hochholzer W, et al. Vascular risk levels affect the predictive value of platelet reactivity for the occurrence of MACE in patients on clopidogrel. Systematic review and meta-analysis of individual patient data. Thromb Haemost. 2016;115:844–855. doi: 10.1160/TH15-09-0742. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
