

Restriction Spectrum Imaging Improves Risk Stratification in Patients with Glioblastoma
- PMID: 28279985
- PMCID: PMC5507368
- DOI: 10.3174/ajnr.A5099
Restriction Spectrum Imaging Improves Risk Stratification in Patients with Glioblastoma
Abstract
Background and purpose: ADC as a marker of tumor cellularity has been promising for evaluating the response to therapy in patients with glioblastoma but does not successfully stratify patients according to outcomes, especially in the upfront setting. Here we investigate whether restriction spectrum imaging, an advanced diffusion imaging model, performed after an operation but before radiation therapy, could improve risk stratification in patients with newly diagnosed glioblastoma relative to ADC.
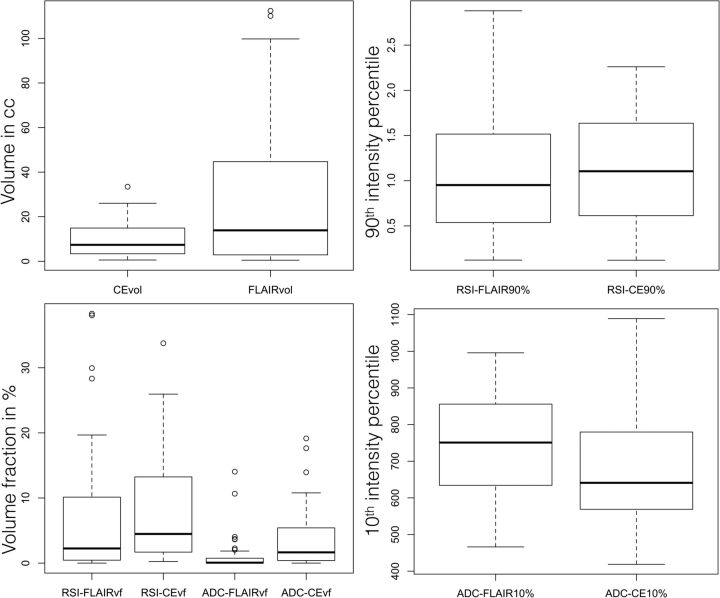
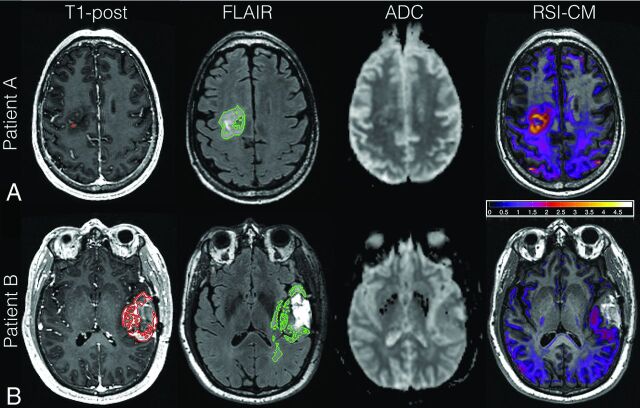
Materials and methods: Pre-radiation therapy diffusion-weighted and structural imaging of 40 patients with glioblastoma were examined retrospectively. Restriction spectrum imaging and ADC-based hypercellularity volume fraction (restriction spectrum imaging-FLAIR volume fraction, restriction spectrum imaging-contrast-enhanced volume fraction, ADC-FLAIR volume fraction, ADC-contrast-enhanced volume fraction) and intensities (restriction spectrum imaging-FLAIR 90th percentile, restriction spectrum imaging-contrast-enhanced 90th percentile, ADC-FLAIR 10th percentile, ADC-contrast-enhanced 10th percentile) within the contrast-enhanced and FLAIR hyperintensity VOIs were calculated. The association of diffusion imaging metrics, contrast-enhanced volume, and FLAIR hyperintensity volume with progression-free survival and overall survival was evaluated by using Cox proportional hazards models.
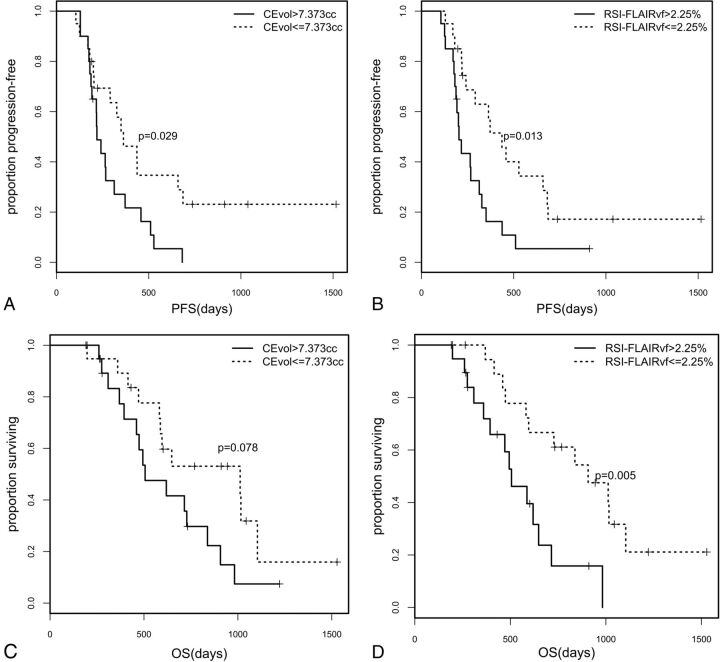
Results: Among the diffusion metrics, restriction spectrum imaging-FLAIR volume fraction was the strongest prognostic metric of progression-free survival (P = .036) and overall survival (P = .007) in a multivariate Cox proportional hazards analysis, with higher values indicating earlier progression and shorter survival. Restriction spectrum imaging-FLAIR 90th percentile was also associated with overall survival (P = .043), with higher intensities, indicating shorter survival. None of the ADC metrics were associated with progression-free survival/overall survival. Contrast-enhanced volume exhibited a trend toward significance for overall survival (P = .063).
Conclusions: Restriction spectrum imaging-derived cellularity in FLAIR hyperintensity regions may be a more robust prognostic marker than ADC and conventional imaging for early progression and poorer survival in patients with glioblastoma. However, future studies with larger samples are needed to explore its predictive ability.
© 2017 by American Journal of Neuroradiology.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. ; European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups, National Cancer Institute of Canada Clinical Trials. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987–96 10.1056/NEJMoa043330 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical