

Cost-Effectiveness Analysis of Quadripolar Versus Bipolar Left Ventricular Leads for Cardiac Resynchronization Defibrillator Therapy in a Large, Multicenter UK Registry
- PMID: 28280785
- PMCID: PMC5328196
- DOI: 10.1016/j.jacep.2016.04.009
Cost-Effectiveness Analysis of Quadripolar Versus Bipolar Left Ventricular Leads for Cardiac Resynchronization Defibrillator Therapy in a Large, Multicenter UK Registry
Abstract
Objectives: The objective of this study was to evaluate the cost-effectiveness of quadripolar versus bipolar cardiac resynchronization defibrillator therapy systems.
Background: Quadripolar left ventricular (LV) leads for cardiac resynchronization therapy reduce phrenic nerve stimulation (PNS) and are associated with reduced mortality compared with bipolar leads.
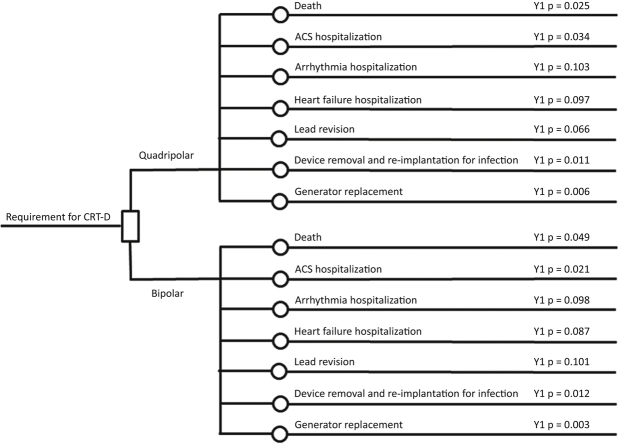
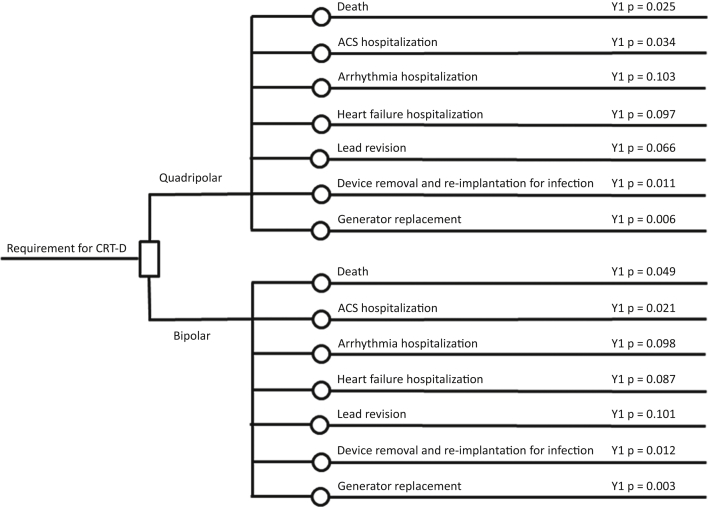
Methods: A total of 606 patients received implants at 3 UK centers (319 Q, 287 B), between 2009 and 2014; mean follow-up was 879 days. Rehospitalization episodes were costed at National Health Service national tariff rates, and EQ-5D utility values were applied to heart failure admissions, acute coronary syndrome events, and mortality data, which were used to estimate quality-adjusted life-year differences over 5 years.
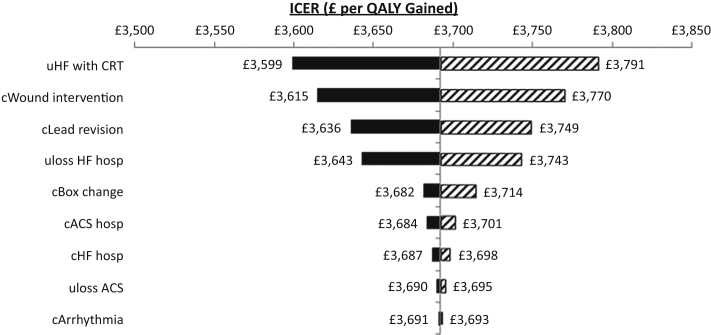
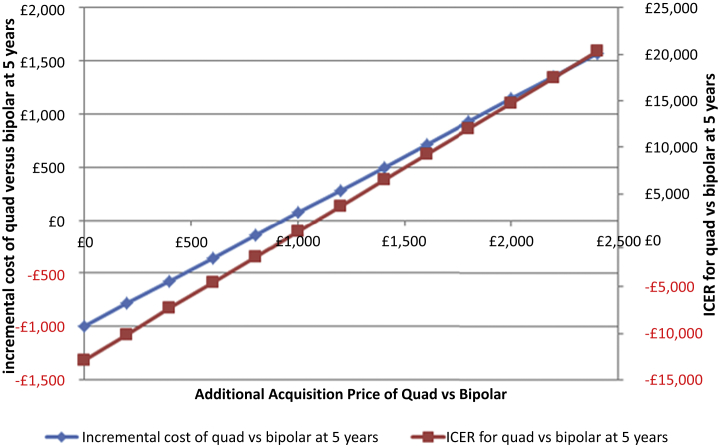
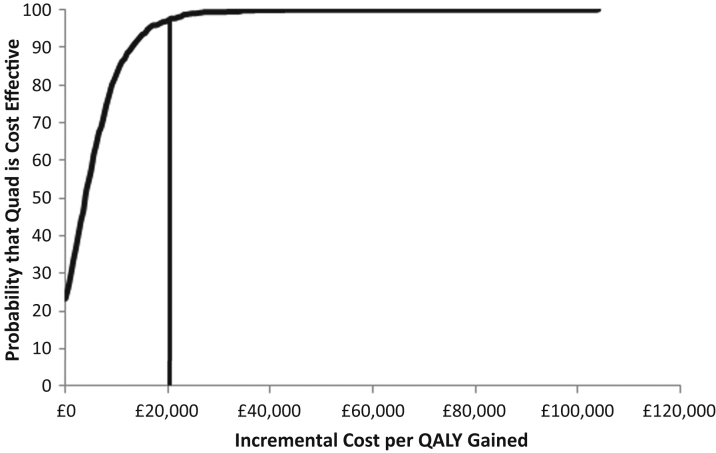
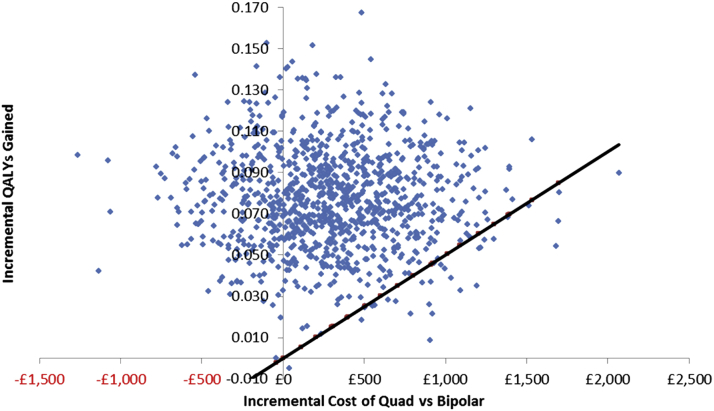
Results: Groups were matched with regard to age and sex. Patients with quadripolar implants had a lower rate of hospitalization than those with bipolar implants (42.6% vs. 55.4%; p = 0.002). This was primarily driven by fewer hospital readmissions for heart failure (51 [16%] vs. 75 [26.1%], respectively, for quadripolar vs. bipolar implants; p = 0.003) and generator replacements (9 [2.8%] vs. 19 [6.6%], respectively; p = 0.03). Hospitalization for suspected acute coronary syndrome, arrhythmia, device explantation, and lead revisions were similar. This lower health-care utilization cost translated into a cumulative 5-year cost saving for patients with quadripolar systems where the acquisition cost was <£932 (US $1,398) compared with bipolar systems. Probabilistic sensitivity analysis results mirrored the deterministic calculations. For the average additional price of £1,200 (US $1,800) over a bipolar system, the incremental cost-effective ratio was £3,692 per quality-adjusted life-year gained (US $5,538), far below the usual willingness-to-pay threshold of £20,000 (US $30,000).
Conclusions: In a UK health-care 5-year time horizon, the additional purchase price of quadripolar cardiac resynchronization defibrillator therapy systems is largely offset by lower subsequent event costs up to 5 years after implantation, which makes this technology highly cost-effective compared with bipolar systems.
Keywords: ACS, acute coronary syndrome; CRT, cardiac resynchronization therapy; CRTD, cardiac resynchronization defibrillator therapy device; HF, heart failure; ICER, incremental cost-effectiveness ratio; LV, left ventricular; NHS, National Health Service; NICE, National Institute for Health and Care Excellence; PNS, phrenic nerve stimulation; QALY, quality-adjusted life-year; cardiac resynchronization therapy; cost-effectiveness; implantable cardiac defibrillator; left ventricular pacing; quadripolar lead.
Figures
Similar articles
-
Cardiac Resynchronization Therapy Delivered Via a Multipolar Left Ventricular Lead is Associated with Reduced Mortality and Elimination of Phrenic Nerve Stimulation: Long-Term Follow-Up from a Multicenter Registry.J Cardiovasc Electrophysiol. 2015 May;26(5):540-6. doi: 10.1111/jce.12625. Epub 2015 Mar 5. J Cardiovasc Electrophysiol. 2015. PMID: 25631303 Free PMC article.
-
Hospitalization rates and associated cost analysis of cardiac resynchronization therapy with an implantable defibrillator and quadripolar vs. bipolar left ventricular leads: a comparative effectiveness study.Europace. 2015 Jan;17(1):101-7. doi: 10.1093/europace/euu290. Epub 2014 Nov 4. Europace. 2015. PMID: 25371428 Free PMC article.
-
Cost-effectiveness of a risk-stratified approach to cardiac resynchronisation therapy defibrillators (high versus low) at the time of generator change.Heart. 2018 Mar;104(5):416-422. doi: 10.1136/heartjnl-2017-311749. Epub 2017 Sep 29. Heart. 2018. PMID: 28970277
-
Economic Considerations of Cardiovascular Implantable Electronic Devices for The Treatment of Heart Failure.Curr Heart Fail Rep. 2024 Jun;21(3):186-193. doi: 10.1007/s11897-024-00664-y. Epub 2024 Apr 25. Curr Heart Fail Rep. 2024. PMID: 38662154 Review.
-
Bipolar versus quadripolar left ventricular leads for cardiac resynchronization therapy: evidence to date.Expert Rev Cardiovasc Ther. 2021 Dec;19(12):1075-1084. doi: 10.1080/14779072.2021.2013813. Expert Rev Cardiovasc Ther. 2021. PMID: 34865590 Review.
Cited by
-
Multipoint left ventricular pacing as an addition to cardiac resynchronization therapy: a bridge to the holy grail?Am J Cardiovasc Dis. 2021 Aug 15;11(4):429-440. eCollection 2021. Am J Cardiovasc Dis. 2021. PMID: 34548940 Free PMC article. Review.
-
Impact of quadripolar LV leads on heart failure hospitalization rates among patients implanted with CRT-D: data from the Israeli ICD Registry.J Interv Card Electrophysiol. 2018 Jan;51(1):5-12. doi: 10.1007/s10840-017-0305-z. Epub 2017 Dec 23. J Interv Card Electrophysiol. 2018. PMID: 29274032
-
Croatian National Data and Comparison with European Practice: Data from the Cardiac Resynchronization Therapy Survey II Multicenter Registry.Cardiol Res Pract. 2018 Oct 25;2018:3479846. doi: 10.1155/2018/3479846. eCollection 2018. Cardiol Res Pract. 2018. PMID: 30498599 Free PMC article.
-
Big Data and Real-World Data based Cost-Effectiveness Studies and Decision-making Models: A Systematic Review and Analysis.Front Pharmacol. 2021 Oct 19;12:700012. doi: 10.3389/fphar.2021.700012. eCollection 2021. Front Pharmacol. 2021. PMID: 34737696 Free PMC article.
-
An active fixation quadripolar left ventricular lead for cardiac resynchronization therapy with reduced postoperative complication rates.J Cardiovasc Electrophysiol. 2022 Mar;33(3):458-463. doi: 10.1111/jce.15346. Epub 2022 Jan 11. J Cardiovasc Electrophysiol. 2022. PMID: 34968010 Free PMC article.
References
-
- Boriani G., Biffi M., Martignani C. Is cardiac resynchronization therapy cost-effective? Europace. 2009;11(Suppl 5):v93–v97. - PubMed
-
- Cleland J.G.F., Daubert J.-C., Erdmann E. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–1549. - PubMed
-
- Brignole M., Auricchio A., Baron-Esquivias G. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association. Eur Heart J. 2013;34:2281–2329. - PubMed
-
- Bristow M.R., Saxon L.A., Boehmer J. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140–2150. - PubMed
-
- Daubert J.-C., Saxon L., Adamson P.B. 2012 EHRA/HRS expert consensus statement on cardiac resynchronization therapy in heart failure: implant and follow-up recommendations and management. Europace. 2012;14:1236–1286. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
