

Inhibition of Interleukin 17-A but not Interleukin-17F Signaling Lowers Blood Pressure and Reduces End-organ Inflammation in Angiotensin II-induced Hypertension
- PMID: 28280792
- PMCID: PMC5337944
- DOI: 10.1016/j.jacbts.2016.07.009
Inhibition of Interleukin 17-A but not Interleukin-17F Signaling Lowers Blood Pressure and Reduces End-organ Inflammation in Angiotensin II-induced Hypertension
Abstract
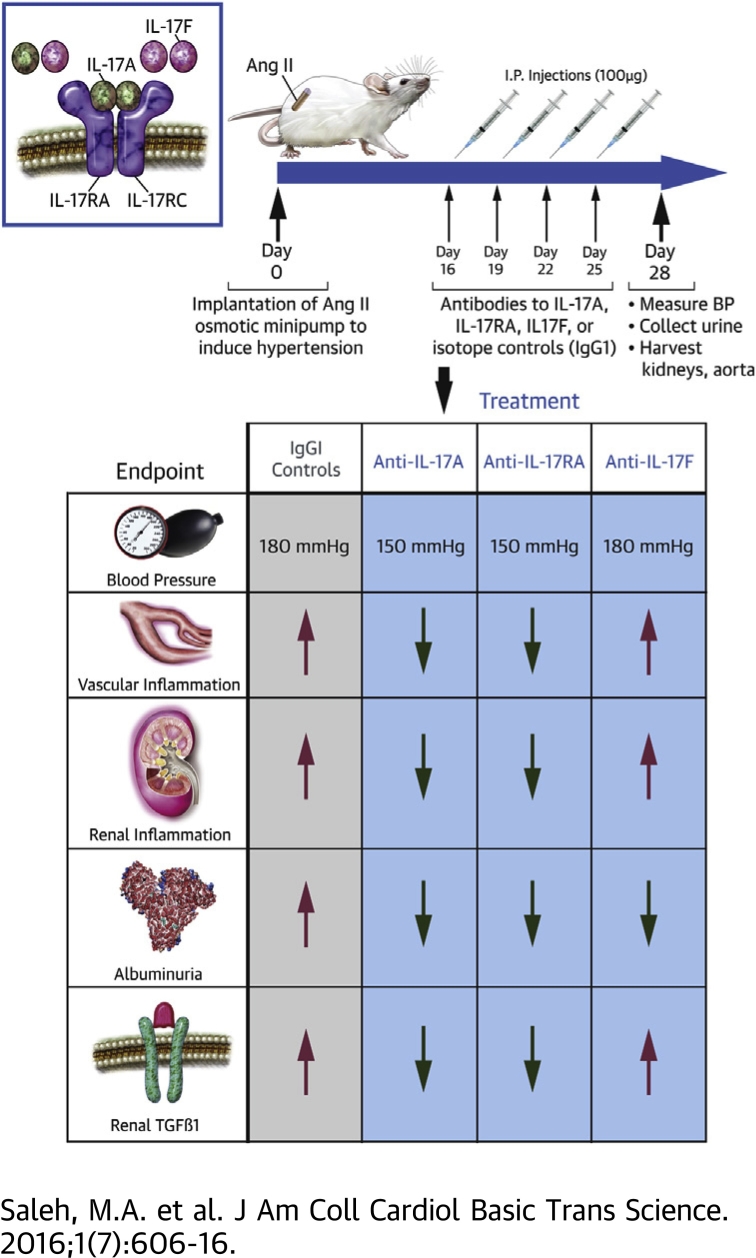
Objectives: To characterize the T cell subsets producing interleukin 17 (IL-17) isoforms A and F in hypertensive kidneys and vessels and determine whether inhibition of IL-17 signaling lowers blood pressure and end-organ damage in a mouse model of hypertension.
Background: T cell derived cytokines play a central role in the pathophysiology of hypertension and contribute to end-organ dysfunction. We previously showed that mice genetically deficient in IL-17A exhibited blunted hypertension and reduced renal and vascular dysfunction in response to angiotensin II (Ang II) infusion. Monoclonal antibodies to IL-17 isoforms or the IL-17 receptor are emerging as novel therapeutics for psoriasis and related autoimmune disorders.
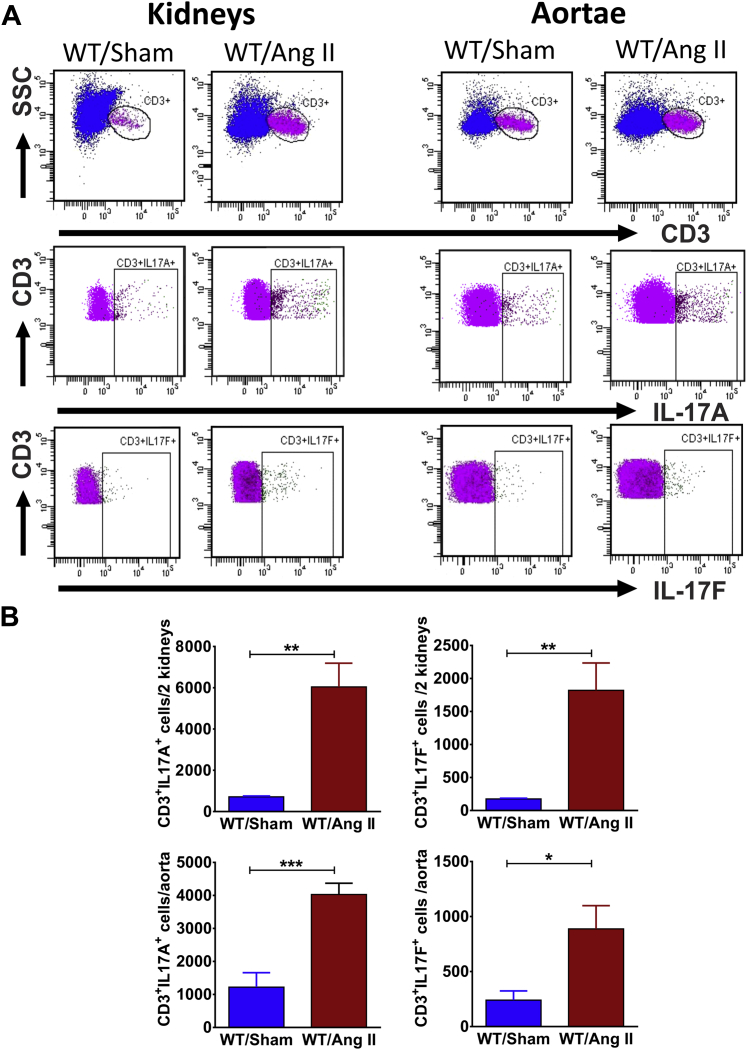
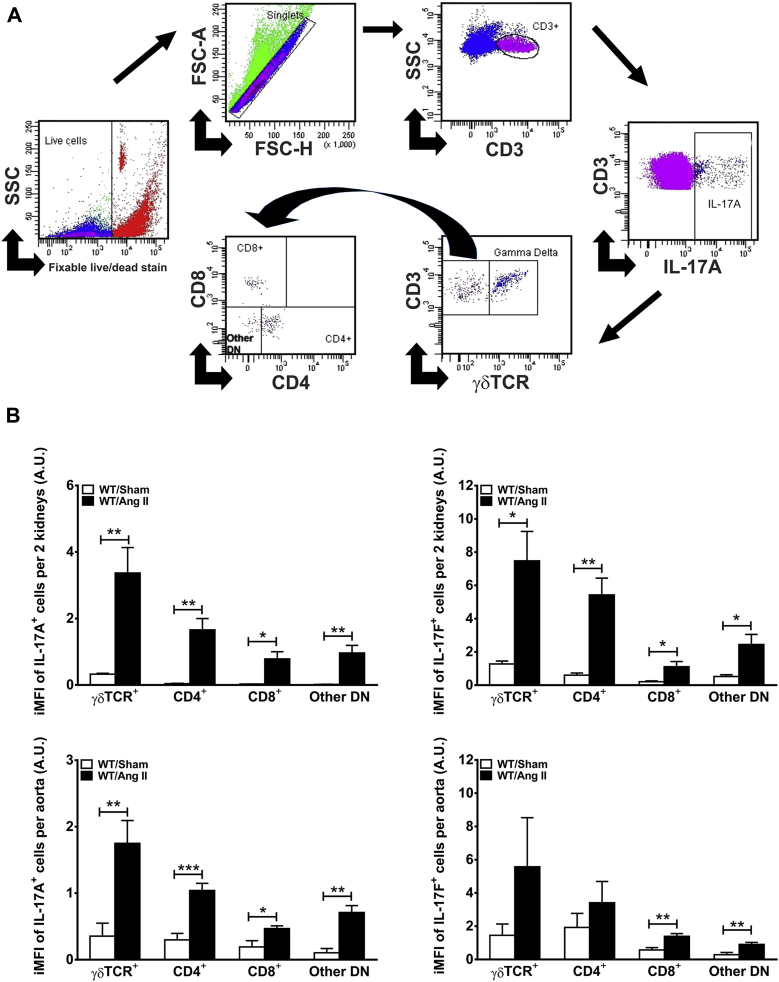
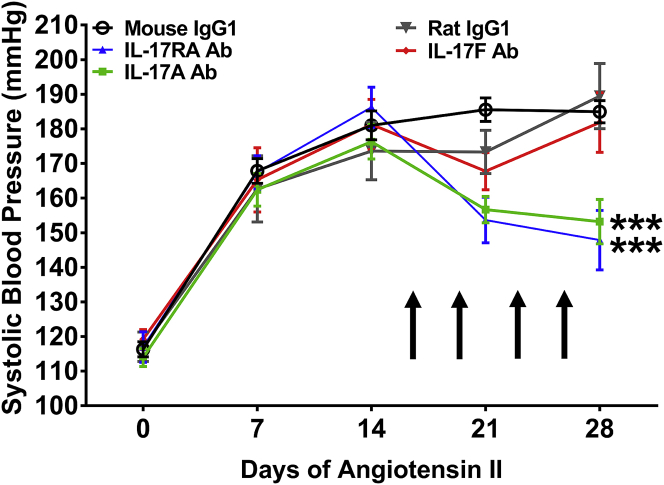
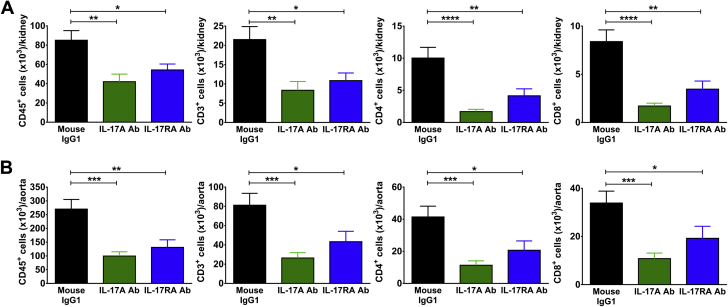
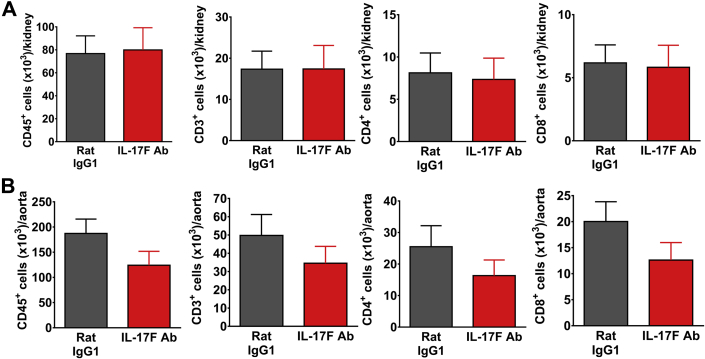
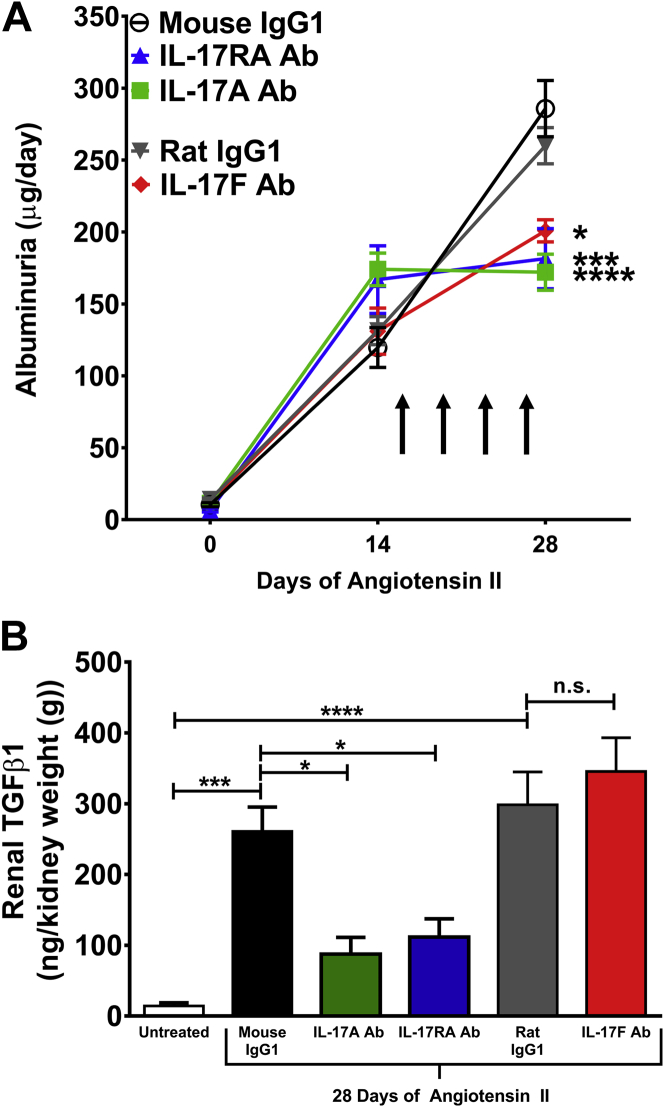
Methods and results: Mice were infused with Ang II for 4 weeks to induce hypertension. Using flow cytometry and intracellular staining, we determined that the primary T cell subsets producing IL-17A and IL-17F in the kidney and aorta are gamma delta (γδ) T cells and CD4+ T helper 17 (TH17) cells. Monoclonal antibodies were administered twice weekly starting 2 weeks after the onset of Ang II infusion. Antibodies to IL-17A or the IL-17 receptor A subunit (IL-17RA), but not IL-17F, lowered blood pressure by 30 mmHg, attenuated renal and vascular lymphocyte infiltration, and reduced renal transforming growth factor beta (TGFβ) levels (a marker of renal fibrosis) compared to control IgG1 antibodies. Inhibition of IL-17 signaling also blunted the progression of albuminuria.
Conclusions: Monoclonal antibodies to IL-17A or IL-17RA, but not IL-17F, may be a useful adjunct treatment for hypertension and the associated end-organ dysfunction.
Keywords: T lymphocytes; angiotensin II; gamma delta T cells; hypertension; interleukin 17A; interleukin 17F; interleukin 17RA receptor.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
