

Gene-to-gene interactions regulate endogenous pain modulation in fibromyalgia patients and healthy controls-antagonistic effects between opioid and serotonin-related genes
- PMID: 28282362
- PMCID: PMC5472004
- DOI: 10.1097/j.pain.0000000000000896
Gene-to-gene interactions regulate endogenous pain modulation in fibromyalgia patients and healthy controls-antagonistic effects between opioid and serotonin-related genes
Abstract
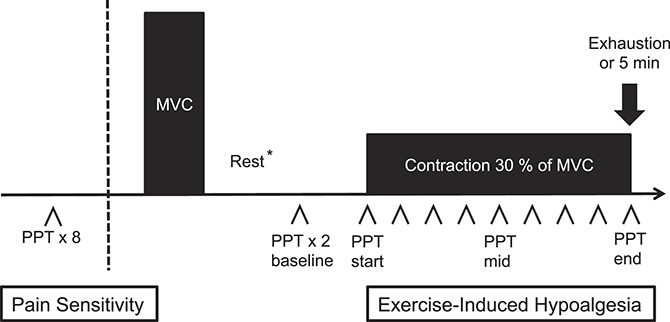
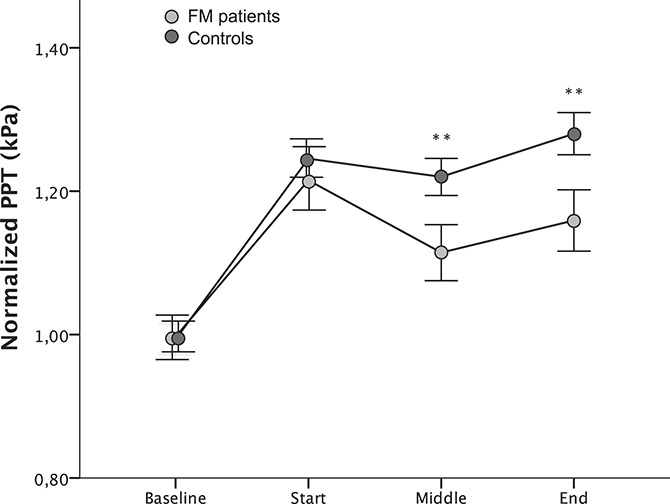
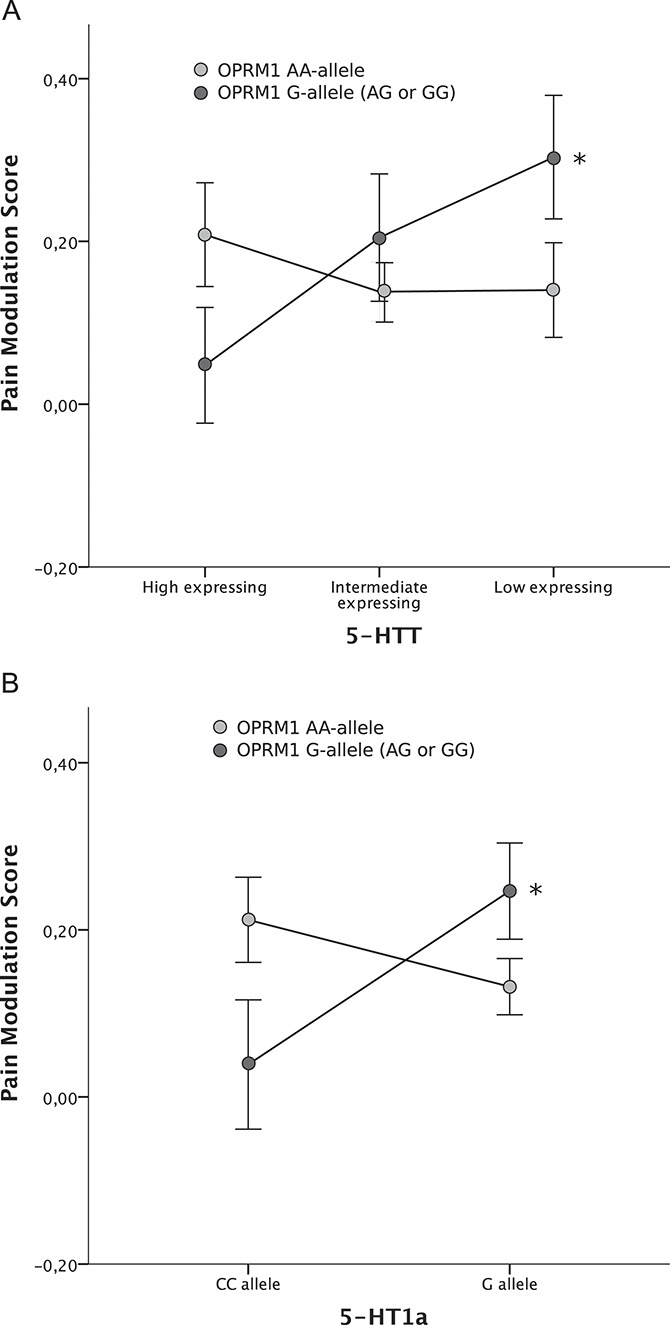
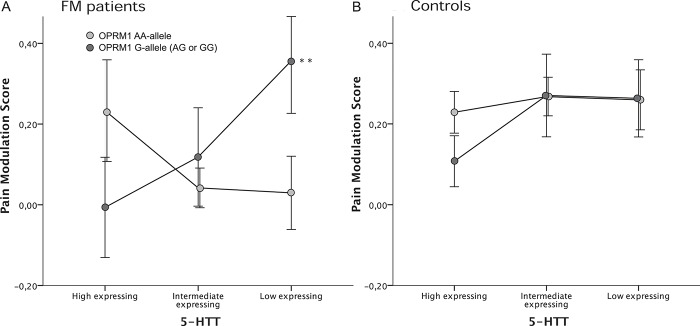
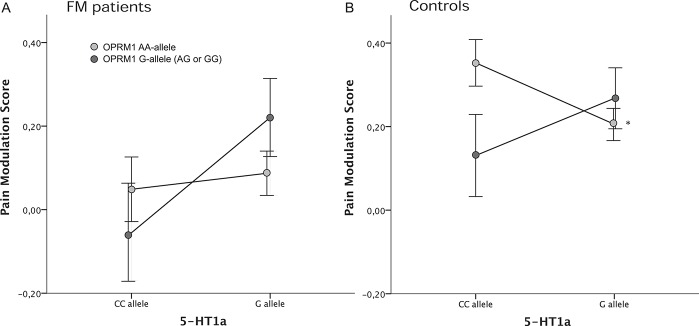
Chronic pain is associated with dysfunctional endogenous pain modulation, involving both central opioid and serotonergic (5-HT) signaling. Fibromyalgia (FM) is a chronic pain syndrome, characterized by widespread musculoskeletal pain and reduced exercise-induced hypoalgesia (EIH). In this study, we assessed the effects of 3 functional genetic polymorphisms on EIH in 130 patients with FM and 132 healthy controls. Subjects were genotyped regarding the mu-opioid receptor (OPRM1) gene (rs1799971), the serotonin transporter (5-HTT) gene (5-HTTLPR/rs25531), and the serotonin-1a receptor (5-HT1a) gene (rs6296). The patients with FM had increased pain sensitivity and reduced EIH compared with healthy controls. None of the polymorphisms had an effect on EIH on their own. We found significant gene-to-gene interactions between OPRM1 x 5-HTT and OPRM1 x 5-HT1a regarding activation of EIH, with no statistically significant difference between groups. Better EIH was found in individuals with genetically inferred strong endogenous opioid signaling (OPRM1 G) in combination with weak 5-HT tone (5-HTT low/5-HT1a G), compared with strong 5-HT tone (5-HTT high/5-HT1a CC). Based on the proposed mechanisms of these genetic variants, the findings indicate antagonistic interactions between opioid and serotonergic mechanisms during EIH. Moreover, despite different baseline pain level, similar results were detected in FM and controls, not supporting an altered interaction between opioid and 5-HT mechanisms as the basis for dysfunction of EIH in patients with FM. In summary, our results suggest that, by genetic association, the mu-opioid receptor interacts with 2 major serotonergic structures involved in 5-HT reuptake and release, to modulate EIH.
Figures
Similar articles
-
The OPRM1 gene and interactions with the 5-HT1a gene regulate conditioned pain modulation in fibromyalgia patients and healthy controls.PLoS One. 2022 Nov 7;17(11):e0277427. doi: 10.1371/journal.pone.0277427. eCollection 2022. PLoS One. 2022. PMID: 36342939 Free PMC article.
-
Serotonergic gene-to-gene interaction is associated with mood and GABA concentrations but not with pain-related cerebral processing in fibromyalgia subjects and healthy controls.Mol Brain. 2021 May 12;14(1):81. doi: 10.1186/s13041-021-00789-4. Mol Brain. 2021. PMID: 33980291 Free PMC article.
-
Polymorphisms of the μ-opioid receptor gene influence cerebral pain processing in fibromyalgia.Eur J Pain. 2021 Feb;25(2):398-414. doi: 10.1002/ejp.1680. Epub 2020 Nov 2. Eur J Pain. 2021. PMID: 33064887 Free PMC article.
-
Genetics of the serotonergic system in suicidal behavior.J Psychiatr Res. 2003 Sep-Oct;37(5):375-86. doi: 10.1016/s0022-3956(03)00048-7. J Psychiatr Res. 2003. PMID: 12849930 Review.
-
Role of the 5-HTTLPR and SNP Promoter Polymorphisms on Serotonin Transporter Gene Expression: a Closer Look at Genetic Architecture and In Vitro Functional Studies of Common and Uncommon Allelic Variants.Mol Neurobiol. 2016 Oct;53(8):5510-26. doi: 10.1007/s12035-015-9409-6. Epub 2015 Oct 13. Mol Neurobiol. 2016. PMID: 26464328 Review.
Cited by
-
Endogenous Opioids and Exercise-Related Hypoalgesia: Modern Models, Measurement, and Mechanisms of Action.Adv Neurobiol. 2024;35:137-155. doi: 10.1007/978-3-031-45493-6_8. Adv Neurobiol. 2024. PMID: 38874722
-
Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update.Int J Mol Sci. 2021 Apr 9;22(8):3891. doi: 10.3390/ijms22083891. Int J Mol Sci. 2021. PMID: 33918736 Free PMC article. Review.
-
Exercise-induced pain and analgesia? Underlying mechanisms and clinical translation.Pain. 2018 Sep;159 Suppl 1(Suppl 1):S91-S97. doi: 10.1097/j.pain.0000000000001235. Pain. 2018. PMID: 30113953 Free PMC article. Review.
-
The effects of a 15-week physical exercise intervention on pain modulation in fibromyalgia: Increased pain-related processing within the cortico-striatal- occipital networks, but no improvement of exercise-induced hypoalgesia.Neurobiol Pain. 2023 Jan 6;13:100114. doi: 10.1016/j.ynpai.2023.100114. eCollection 2023 Jan-Jul. Neurobiol Pain. 2023. PMID: 36660198 Free PMC article.
-
Biopsychosocial contributors to irritability in individuals with shoulder or low back pain.J Man Manip Ther. 2024 Aug;32(4):400-411. doi: 10.1080/10669817.2023.2294679. Epub 2023 Dec 18. J Man Manip Ther. 2024. PMID: 38108631 Free PMC article.
References
-
- Ablin JN, Buskila D. Update on the genetics of the fibromyalgia syndrome. Best Pract Res Clin Rheumatol 2015;29:20–8. - PubMed
-
- Bardin L, Colpaert FC. Role of spinal 5-HT(1A) receptors in morphine analgesia and tolerance in rats. Eur J Pain 2004;8:253–61. - PubMed
-
- Benarroch EE. Descending monoaminergic pain modulation: bidirectional control and clinical relevance. Neurology 2008;71:217–21. - PubMed
-
- Bennett R. The Fibromyalgia Impact Questionnaire (FIQ): a review of its development, current version, operating characteristics and uses. Clin Exp Rheumatol 2005;23(5 suppl 39):S154–162. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
