

A human judgment approach to epidemiological forecasting
- PMID: 28282375
- PMCID: PMC5345757
- DOI: 10.1371/journal.pcbi.1005248
A human judgment approach to epidemiological forecasting
Abstract
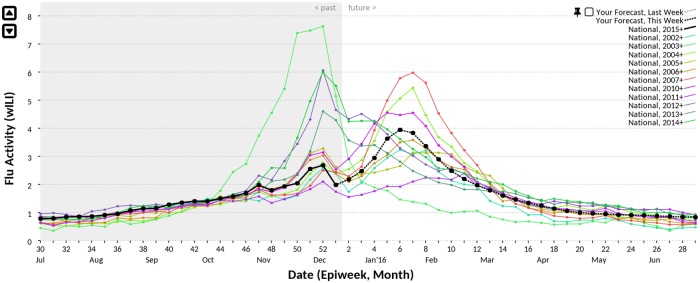
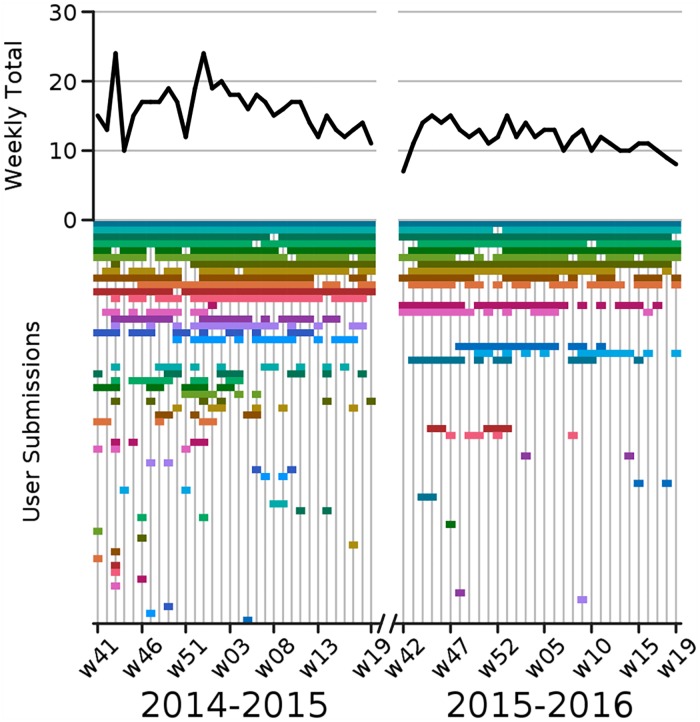
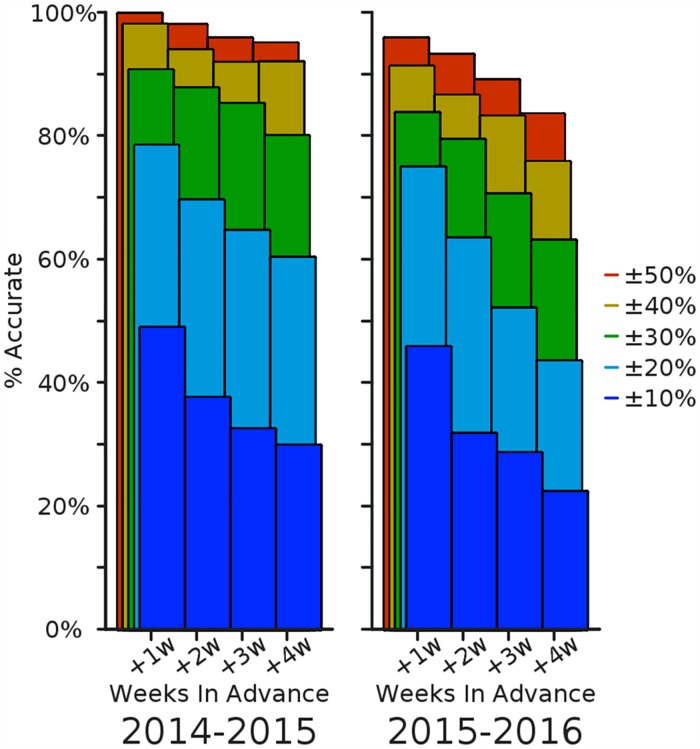
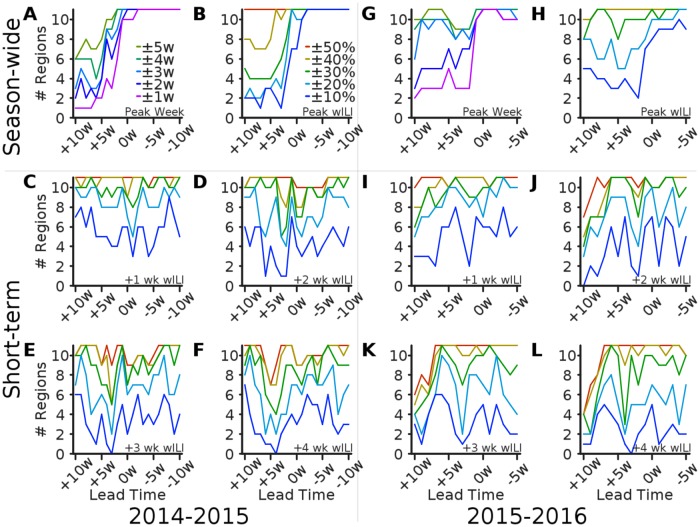
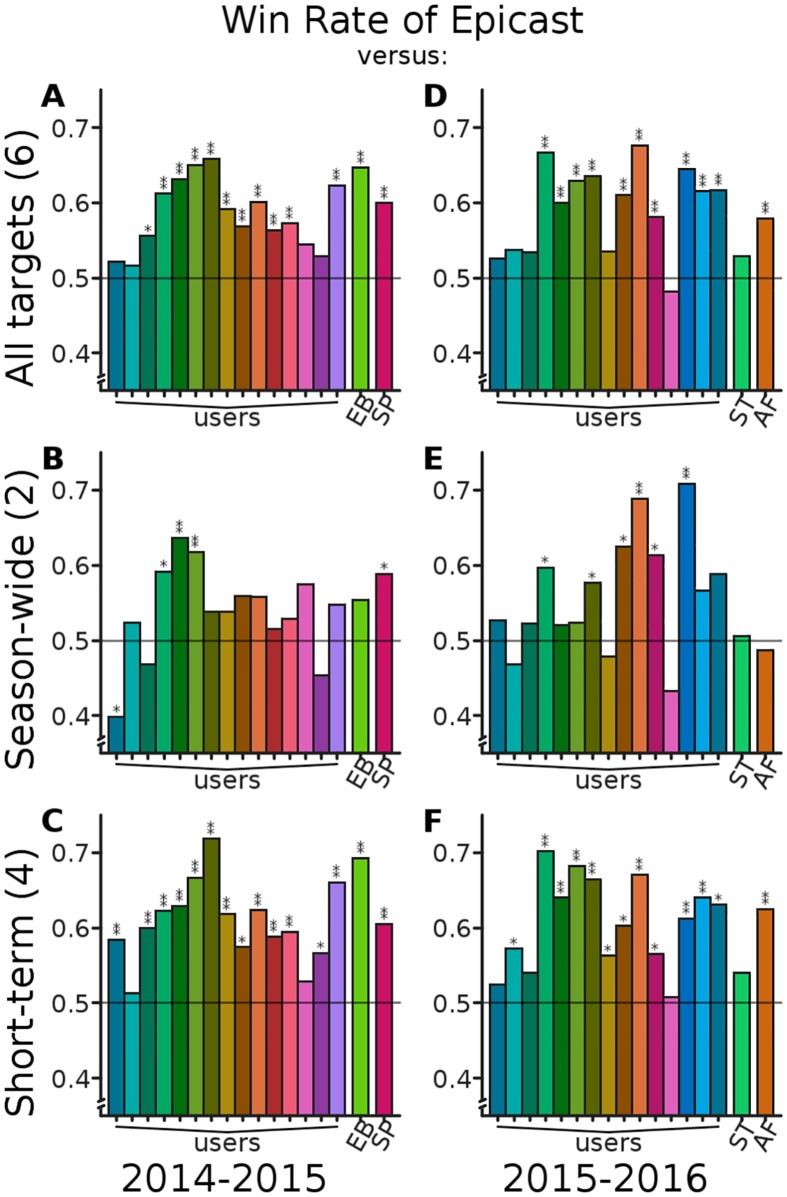
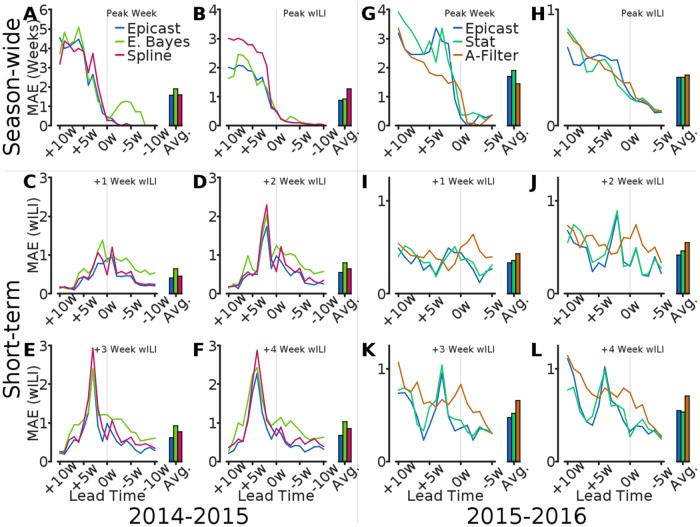
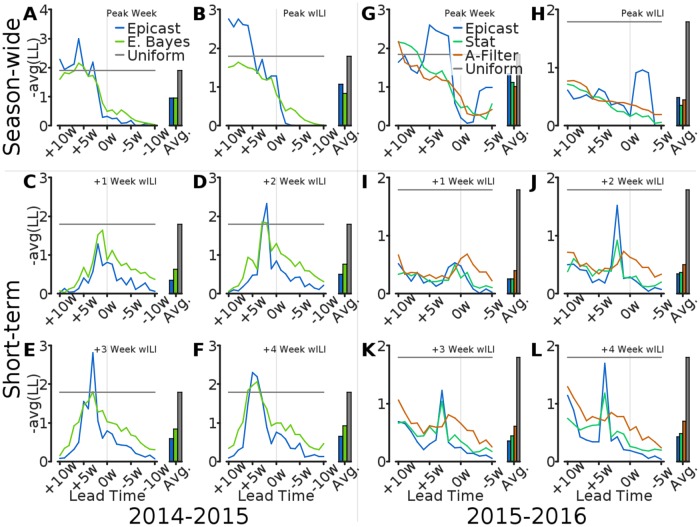
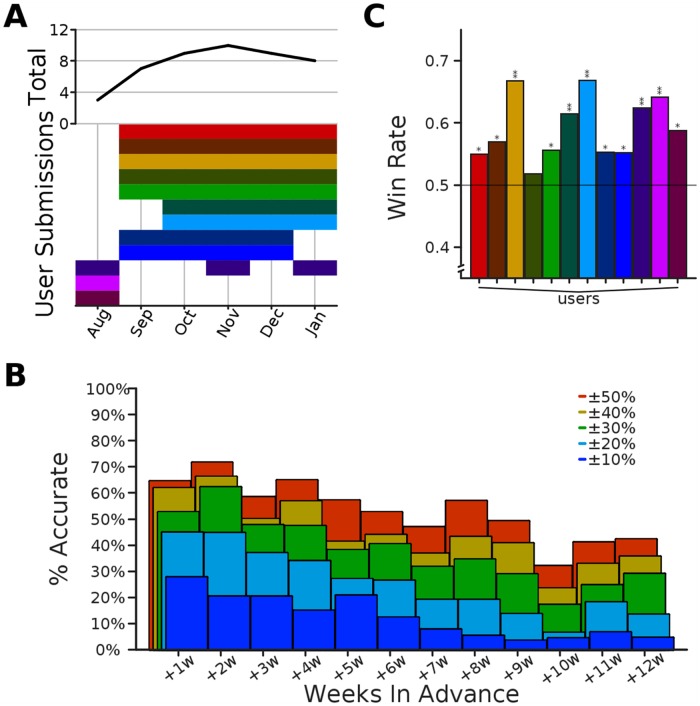
Infectious diseases impose considerable burden on society, despite significant advances in technology and medicine over the past century. Advanced warning can be helpful in mitigating and preparing for an impending or ongoing epidemic. Historically, such a capability has lagged for many reasons, including in particular the uncertainty in the current state of the system and in the understanding of the processes that drive epidemic trajectories. Presently we have access to data, models, and computational resources that enable the development of epidemiological forecasting systems. Indeed, several recent challenges hosted by the U.S. government have fostered an open and collaborative environment for the development of these technologies. The primary focus of these challenges has been to develop statistical and computational methods for epidemiological forecasting, but here we consider a serious alternative based on collective human judgment. We created the web-based "Epicast" forecasting system which collects and aggregates epidemic predictions made in real-time by human participants, and with these forecasts we ask two questions: how accurate is human judgment, and how do these forecasts compare to their more computational, data-driven alternatives? To address the former, we assess by a variety of metrics how accurately humans are able to predict influenza and chikungunya trajectories. As for the latter, we show that real-time, combined human predictions of the 2014-2015 and 2015-2016 U.S. flu seasons are often more accurate than the same predictions made by several statistical systems, especially for short-term targets. We conclude that there is valuable predictive power in collective human judgment, and we discuss the benefits and drawbacks of this approach.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
