

Association of Provider Specialty and Multidisciplinary Care With Hepatocellular Carcinoma Treatment and Mortality
- PMID: 28283421
- PMCID: PMC5664153
- DOI: 10.1053/j.gastro.2017.02.040
Association of Provider Specialty and Multidisciplinary Care With Hepatocellular Carcinoma Treatment and Mortality
Abstract
Background & aims: Little is known about provider and health system factors that affect receipt of active therapy and outcomes of patients with hepatocellular carcinoma (HCC). We investigated patient, provider, and health system factors associated with receipt of active HCC therapy and overall survival.
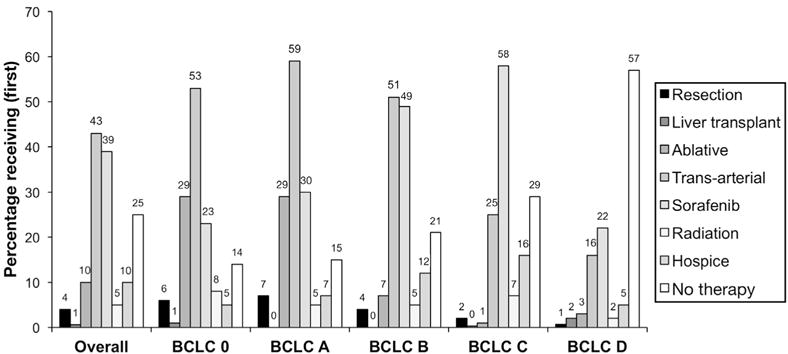
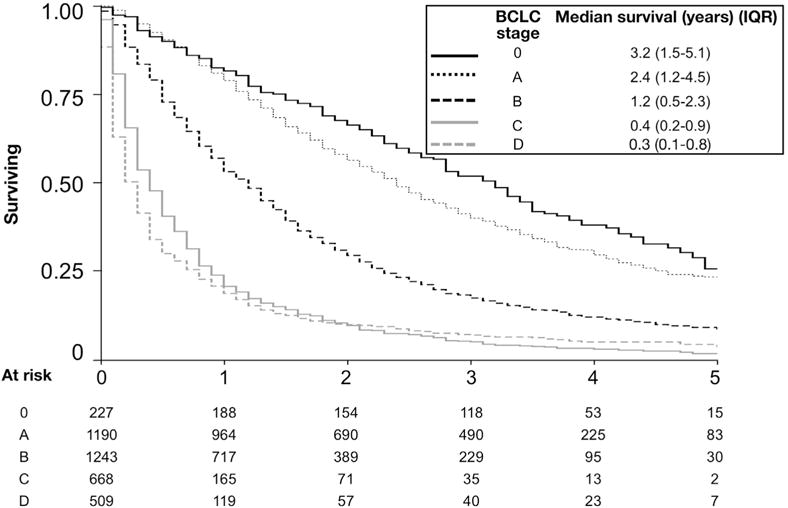
Methods: We performed a national, retrospective cohort study of all patients diagnosed with HCC from January 1, 2008 through December 31, 2010 (n = 3988) and followed through December 31 2014 who received care through the Veterans Administration (128 centers). Outcomes were receipt of active HCC therapy (liver transplantation, resection, local ablation, transarterial therapy, or sorafenib) and overall survival.
Results: In adjusted analyses, receiving care at an academically affiliated Veterans Administration hospital (odds ratio [OR], 1.97; 95% confidence interval [CI], 1.60-2.41) or a multi-specialist evaluation (OR, 1.60; 95% CI, 1.15-2.21), but not review by a multidisciplinary tumor board (OR, 1.19; 95% CI, 0.98-1.46), was associated with a higher likelihood of receiving active HCC therapy. In time-varying Cox proportional hazards models, liver transplantation (hazard ratio [HR], 0.22; 95% CI, 0.16-0.31), liver resection (HR, 0.38; 95% CI, 0.28-0.52), ablative therapy (HR, 0.63; 95% CI, 0.52-0.76), and transarterial therapy (HR, 0.83; 95% CI, 0.74-0.92) were associated with reduced mortality. Subspecialist care by hepatologists (HR, 0.70; 95% CI, 0.63-0.78), medical oncologists (HR, 0.82; 95% CI, 0.74-0.91), or surgeons (HR, 0.79; 95% CI, 0.71-0.89) within 30 days of HCC diagnosis, and review by a multidisciplinary tumor board (HR, 0.83; 95% CI, 0.77-0.90), were associated with reduced mortality.
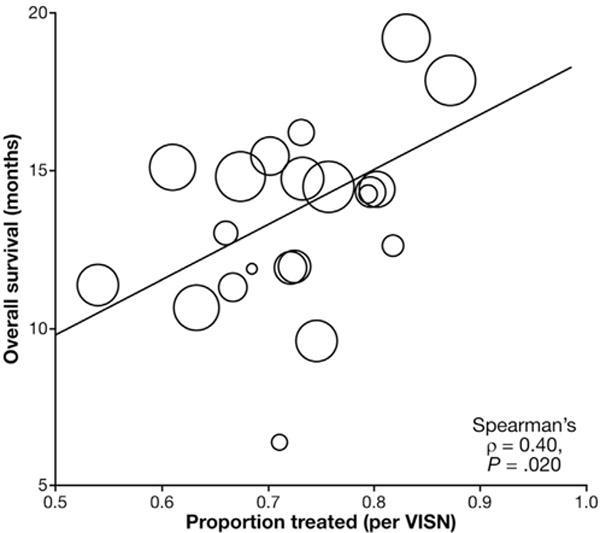
Conclusions: In a retrospective cohort study of almost 4000 patients with HCC cared for at VA centers, geographic, provider, and system differences in receipt of active HCC therapy are associated with patient survival. Multidisciplinary methods of care delivery for HCC should be prospectively evaluated and standardized to improve access to HCC therapy and optimize outcomes.
Keywords: Liver Cancer; Population; Quality; Risk Factor.
Copyright © 2017 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors disclose no conflicts.
Figures
Comment in
-
Multidisciplinary Care in Hepatocellular Carcinoma: Where Do We Go From Here?Gastroenterology. 2017 Jun;152(8):1823-1825. doi: 10.1053/j.gastro.2017.04.029. Epub 2017 Apr 28. Gastroenterology. 2017. PMID: 28461194 No abstract available.
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0 Cancer incidence and mortality worldwide: IARC CancerBase No. 11. Lyon, France: International Agency for Research on Cancer; 2013. Available at: http://globocan.iarc.fr/ (accessed June 24, 2016)
-
- Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379:1245–1255. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
