

The Incidence and Health Care Resource Burden of the Myelodysplastic Syndromes in Patients in Whom First-Line Hypomethylating Agents Fail
- PMID: 28283585
- PMCID: PMC5388372
- DOI: 10.1634/theoncologist.2016-0211
The Incidence and Health Care Resource Burden of the Myelodysplastic Syndromes in Patients in Whom First-Line Hypomethylating Agents Fail
Abstract
Background: Although hypomethylating agents (HMAs) are effective and approved therapies for patients with myelodysplastic syndromes (MDS), many patients do not benefit from treatment, and nearly all ultimately stop responding to HMAs. The incidence and cost burden of HMA failure are unknown yet needed to appreciate the magnitude and significance of such failure.
Methods: We analyzed a de-identified dataset of over 5 million individuals with private health insurance in the U.S. to estimate MDS incidence, prevalence, and treatments. Based on MDS provider interviews, a conceptual model of MDS patient management was constructed to create a new, claims-relevant and drug development-relevant definition of HMA treatment failure. This algorithm was used to define resource encumbrance of MDS patients in whom HMA treatment failed.
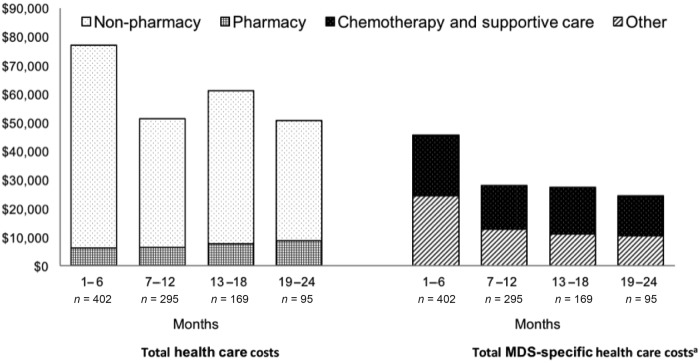
Results: We estimated an MDS incidence rate of ∼70 cases per 100,000 enrollees per year and a prevalence of 155 cases per 100,000 enrollees. The proportion of MDS patients receiving HMA treatment was low (∼3%), and treatment was typically initiated within 1 year of the first MDS claim. Notably, HMA-treated individuals were older and had more comorbidities than the overall MDS cohort. Total health care costs of managing MDS patients after HMA failure were high (∼$77,000 during the first 6 months) and were driven primarily by non-pharmacy costs.
Conclusion: This study quantifies for the first time the burden of significant unmet need in caring for MDS patients following HMA treatment failure. The Oncologist 2017;22:379-385Implications for Practice: U.S.-based treatment patterns among MDS patients demonstrate the significant clinical, financial, and health care burden associated with HMA failure and call for active therapies for this patient population.
Keywords: Cost of illness; Incidence; Myelodysplastic syndromes; Prevalence.
© AlphaMed Press 2017.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
