

What is the Ideal Route of Administration of Tranexamic Acid in TKA? A Randomized Controlled Trial
- PMID: 28283902
- PMCID: PMC5498377
- DOI: 10.1007/s11999-017-5311-z
What is the Ideal Route of Administration of Tranexamic Acid in TKA? A Randomized Controlled Trial
Abstract
Background: TKA commonly involves substantial blood loss and tranexamic acid has been used to reduce blood loss after TKA. Numerous clinical trials have documented the efficacy and safety of intravenous (IV) or intraarticular (IA) use of tranexamic acid. Combined administration of tranexamic acid also has been suggested; however, there is no consensus regarding the ideal route of tranexamic acid administration.
Questions/purposes: (1) To compare the efficacy of tranexamic acid in terms of total blood loss and the allogeneic transfusion rate among three routes of administration: IV alone, IA alone, and combined IV and IA. (2) To compare these regimens in terms of venous thromboembolism (VTE) and the frequency of wound complications.
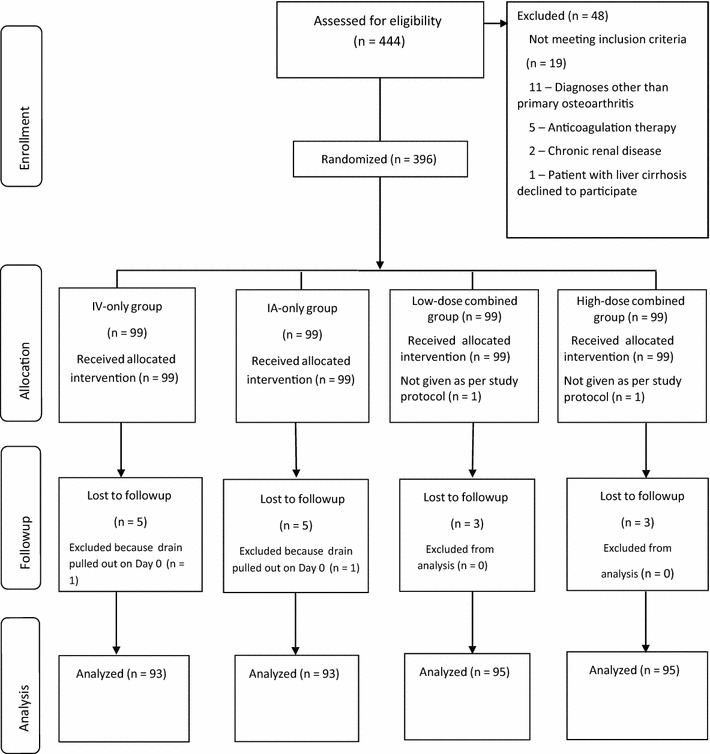
Methods: In total, 376 patients undergoing TKA between March 2014 and March 2015 were randomized to four groups by the route of tranexamic acid administration: IV only, IA only, low-dose combined (IV + IA injection of 1 g), and high-dose combined (IV + IA injection of 2 g). The calculated total blood loss, allogeneic transfusion rate, decrease in hemoglobin, the frequency of symptomatic deep vein thrombosis and pulmonary embolism, wound complications, and periprosthetic joint infection were compared among the groups. Total blood loss was calculated using estimated total body blood volume and hemoglobin loss. The decision regarding when to transfuse was determined based on preset criteria.
Results: The high- and low-dose combined groups and the IA-only group had lower total blood loss (564 ± 242 mL, 642 ± 242 mL, and 633 ± 205 mL, respectively) than the IV-only group (764 ± 217 mL; mean differences = 199 mL [95% CI, 116-283 mL], p < 0.001; 121 mL [95% CI, 38-205 mL], p = 0.001; 131 mL [95% CI, 47-214 mL], p < 0.001); no differences were found among the other three groups. No patients in any study group received an allogeneic transfusion. One patient in the IV-only group had a symptomatic pulmonary embolism develop, but no other symptomatic VTE events occurred in any group. In addition, no differences were observed in wound complications, such as superficial wound necrosis (one patient in the IV-only and the high-dose combined group, respectively) and oozing (IV-only, IA-only, low-dose combined, high-dose combined = 3%, 4%, 4%, and 7%; p = 0.572) between the groups. No patients had a periprosthetic joint infection.
Conclusion: IA tranexamic acid administration further reduces blood loss after TKA in comparison to IV use alone; no additional effect in further reducing blood loss was found in combination with IV tranexamic acid. Appropriately powered studies are needed to confirm the safety of this route of administration as the preferred route of administration in TKA.
Level of evidence: Level I, therapeutic study.
Figures
Comment in
-
CORR Insights®: What is the Ideal Route of Administration of Tranexamic Acid in TKA? A Randomized Controlled Trial.Clin Orthop Relat Res. 2017 Aug;475(8):1997-1998. doi: 10.1007/s11999-017-5322-9. Epub 2017 Mar 23. Clin Orthop Relat Res. 2017. PMID: 28337652 Free PMC article. No abstract available.
Similar articles
-
Combined Intra-Articular and Intravenous Tranexamic Acid Reduces Blood Loss in Total Knee Arthroplasty: A Randomized, Double-Blind, Placebo-Controlled Trial.J Bone Joint Surg Am. 2016 May 18;98(10):835-41. doi: 10.2106/JBJS.15.00810. J Bone Joint Surg Am. 2016. PMID: 27194493 Clinical Trial.
-
Combined Administration of Systemic and Topical Tranexamic Acid for Total Knee Arthroplasty: Can It Be a Better Regimen and Yet Safe? A Randomized Controlled Trial.J Arthroplasty. 2016 Feb;31(2):542-7. doi: 10.1016/j.arth.2015.09.029. Epub 2015 Sep 26. J Arthroplasty. 2016. PMID: 26507526 Clinical Trial.
-
Is combined use of intravenous and intraarticular tranexamic acid superior to intravenous or intraarticular tranexamic acid alone in total knee arthroplasty? A meta-analysis of randomized controlled trials.J Orthop Surg Res. 2017 Apr 18;12(1):61. doi: 10.1186/s13018-017-0559-2. J Orthop Surg Res. 2017. PMID: 28420413 Free PMC article.
-
The efficacy and safety of combined administration of intravenous and topical tranexamic acid in primary total knee arthroplasty: a meta-analysis of randomized controlled trials.BMC Musculoskelet Disord. 2018 Sep 7;19(1):321. doi: 10.1186/s12891-018-2181-9. BMC Musculoskelet Disord. 2018. PMID: 30193586 Free PMC article. Review.
-
Is tranexamic acid clinically effective and safe to prevent blood loss in total knee arthroplasty? A meta-analysis of 34 randomized controlled trials.Eur J Orthop Surg Traumatol. 2015 Apr;25(3):525-41. doi: 10.1007/s00590-014-1568-z. Epub 2014 Nov 28. Eur J Orthop Surg Traumatol. 2015. PMID: 25430635 Review.
Cited by
-
The antifibrinolytic and anti-inflammatory effects of a high initial-dose tranexamic acid in total knee arthroplasty: a randomized controlled trial.Int Orthop. 2020 Mar;44(3):477-486. doi: 10.1007/s00264-019-04469-w. Epub 2019 Dec 26. Int Orthop. 2020. PMID: 31879812 Clinical Trial.
-
Combined Intravenous and Intraarticular Tranexamic Acid Does Not Offer Additional Benefit Compared with Intraarticular Use Alone in Bilateral TKA: A Randomized Controlled Trial.Clin Orthop Relat Res. 2020 Jan;478(1):45-54. doi: 10.1097/CORR.0000000000000942. Clin Orthop Relat Res. 2020. PMID: 31498264 Free PMC article.
-
Is there a maximal effect of tranexamic acid in patients undergoing total knee arthroplasty? A randomized controlled trial.MedComm (2020). 2020 Aug 27;1(2):219-227. doi: 10.1002/mco2.23. eCollection 2020 Sep. MedComm (2020). 2020. PMID: 34766120 Free PMC article.
-
Bipolar vs. monopolar sealer in decreasing blood loss and transfusion rate in patients undergoing two-stage exchange in infected total knee arthroplasty: propensity score-matched study.Arch Orthop Trauma Surg. 2025 Jan 15;145(1):129. doi: 10.1007/s00402-024-05685-9. Arch Orthop Trauma Surg. 2025. PMID: 39812658
-
Low relative muscle volume: Correlation with prevalence of venous thromboembolism following total knee arthroplasty.PLoS One. 2019 Mar 5;14(3):e0210800. doi: 10.1371/journal.pone.0210800. eCollection 2019. PLoS One. 2019. PMID: 30835735 Free PMC article.
References
-
- Astedt B, Liedholm P, Wingerup L. The effect of tranexamic acid on the fibrinolytic activity of vein walls. Ann Chir Gynaecol. 1978;67:203–205. - PubMed
-
- Benoni G, Fredin H. Fibrinolytic inhibition with tranexamic acid reduces blood loss and blood transfusion after knee arthroplasty: a prospective, randomised, double-blind study of 86 patients. J Bone Joint Surg Br. 1996;78:434–440. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
